

Epidemiology risk factors and antifungal resistance patterns of Candida in cancer patients in Jiangxi China
- PMID: 40766085
- PMCID: PMC12321901
- DOI: 10.3389/fmicb.2025.1630226
Epidemiology risk factors and antifungal resistance patterns of Candida in cancer patients in Jiangxi China
Abstract
Background: Candidiasis in cancer patients remains largely unexplored in China. This study examines risk factors and antifungal susceptibility patterns of Candida in cancer patients from Jiangxi, China.
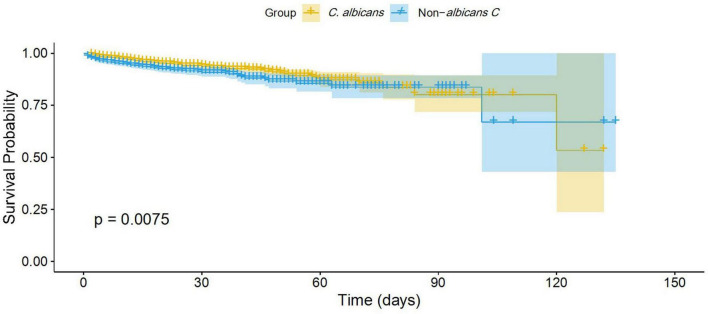
Methods: Clinical and demographic data on Candida in cancer patients (2018-2024) were retrospectively collected at Jiangxi Cancer Hospital, Nanchang, China. Candida distribution across cancers and antifungal susceptibility patterns were analyzed. Risk factors were identified via logistic regression, and antifungal consumption was correlated with Candida distribution. Survival probabilities were compared between patients with C. albicans and those with non-albicans Candida (NAC) infections.
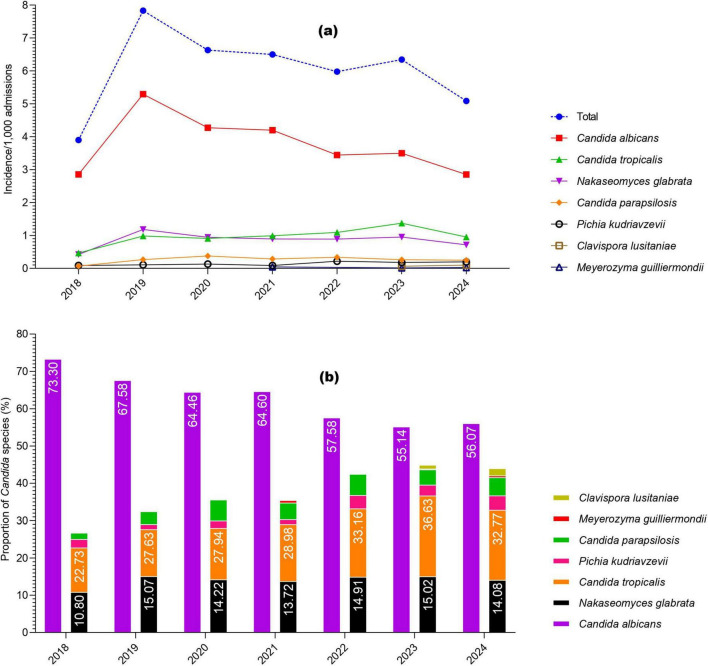
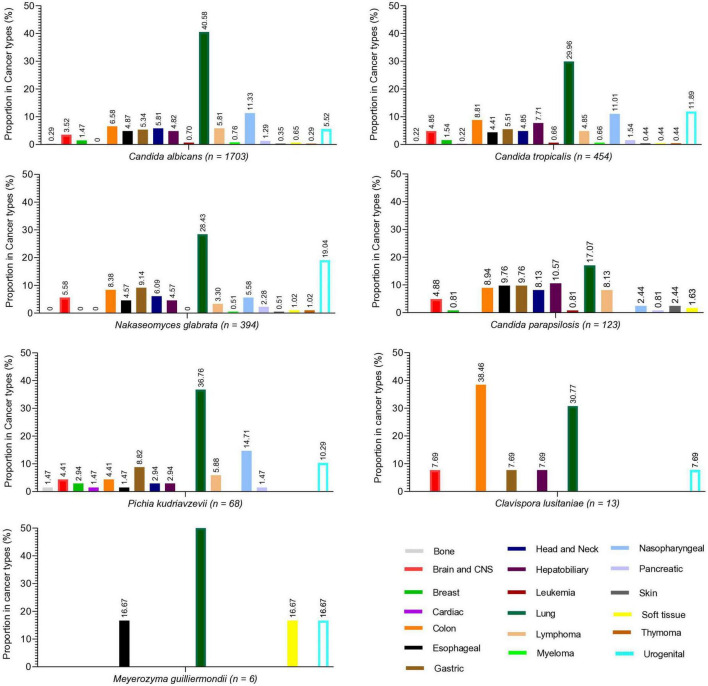
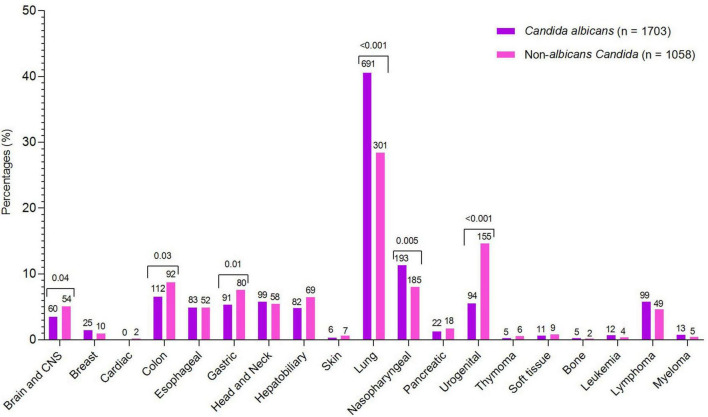
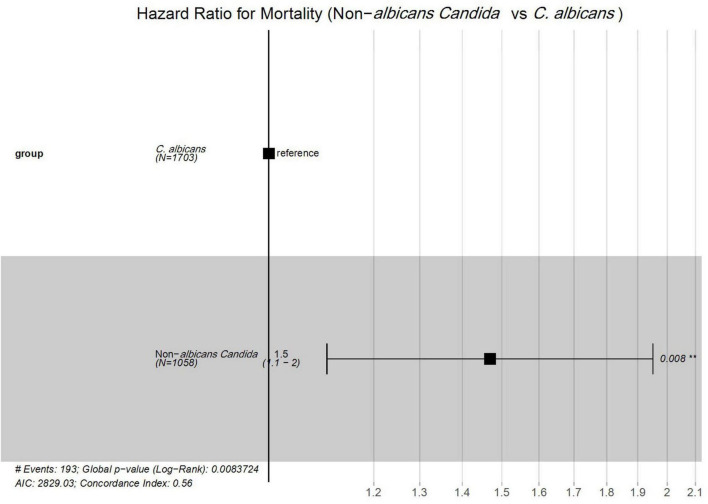
Results: Among 2,761 Candida isolates, 1,703 (61.68%) were C. albicans and 1,058 (38.31%) were NAC, with a year-wise trend showing a decline in C. albicans and a rise in NAC. C. albicans was significantly higher in lung (40.57%) and nasopharyngeal (11.33%) cancers, while NAC were more common in gastric (7.56%), colon (8.69%), and urogenital (14.65%) cancers. NAC risk factors included inappropriate empirical therapy (OR 13.8, P < 0.001), hypoproteinemia (OR 1.35), anemia (OR 1.28), urinary tract infection (OR 1.71), and indwelling catheters (OR 1.27) (all P < 0.05). Radiotherapy, targeted therapy, glucocorticoids, chest tube insertion, and parenteral nutrition were associated with C. albicans (P ≤ 0.01). Amphotericin B (>99%) and echinocandins (>96%) showed the highest efficacy. C. tropicalis displayed notable azole resistance (40.9-74.45%). Caspofungin use negatively correlated with C. albicans (r = -0.84, P = 0.02) and positively with C. tropicalis (r = 0.78, P = 0.04) and N. glabrata (r = 0.85, p = 0.02). NAC infections showed 1.5-fold higher mortality rate than C. albicans (95% CI: 1.1-2.0; P = 0.0075).
Conclusion: These findings may aid healthcare officials in improving Candida management in the region and similar settings.
Keywords: Candida species; antifungal consumption; antifungal resistance; cancer patients; epidemiology and risk factors.
Copyright © 2025 Bilal, Li, Wang, Khan, Shafiq, Yu, Qiu, Lv and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Bilal H., Zhang D., Shafiq M., Khan M. N., Chen C., Khan S., et al. (2023). Six-Year retrospective analysis of epidemiology, risk factors, and antifungal susceptibilities of candidiasis from a tertiary care hospital in South China. Microbiol. Spect. 11:e0070823. 10.1128/spectrum.00708-23 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources