

Clinical Burden and Costs of Anti-Neutrophil Cytoplasmic Antibody-ANCA-Associated Vasculitis: Main Findings from REDCap Registry of a University Hospital in Spain
- PMID: 40766903
- PMCID: PMC12323866
- DOI: 10.2147/CEOR.S529853
Clinical Burden and Costs of Anti-Neutrophil Cytoplasmic Antibody-ANCA-Associated Vasculitis: Main Findings from REDCap Registry of a University Hospital in Spain
Abstract
Purpose: Anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV) are rare chronic autoimmune diseases, potentially fatal, with frequent relapses. They are associated with vital organ damage, especially renal, often resulting in end-stage renal disease. While current standard of care with immunosuppressants has improved renal function and survival, the main risks for patients under life-long immunosuppression are infections and other concomitant diseases. This study evaluated the burden of AAV using patient-level data from a disease-specific registry.
Patients and methods: The cohort of incident AVV patients (2013-2022) in the REDCap registry in a university hospital in Spain was studied. Patients with Granulomatosis with Polyangiitis (GPA), Microscopic Polyangiitis (MPA) and Eosinophilic Granulomatosis with Polyangiitis (EGPA) with at least one year of follow-up (or deceased during the period) were included. Clinical outcomes, including Birmingham Vasculitis Activity Score (BVAS) and healthcare resource consumption were analysed for the first year after diagnosis. Mean annual costs were calculated using unitary costs from the hospital accounting department.
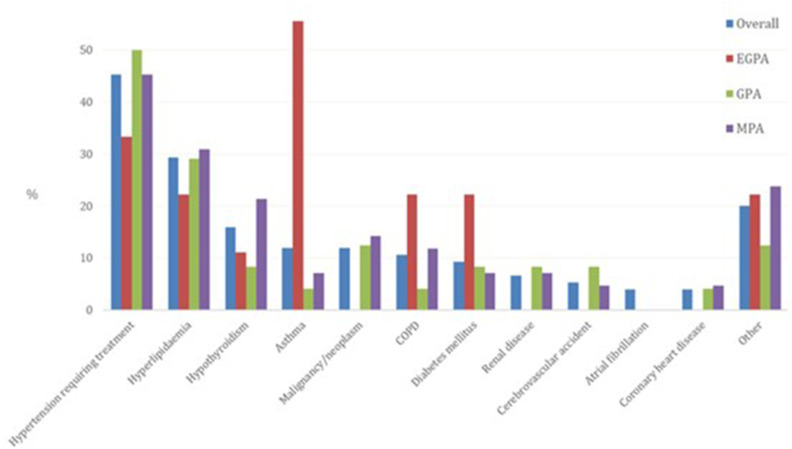
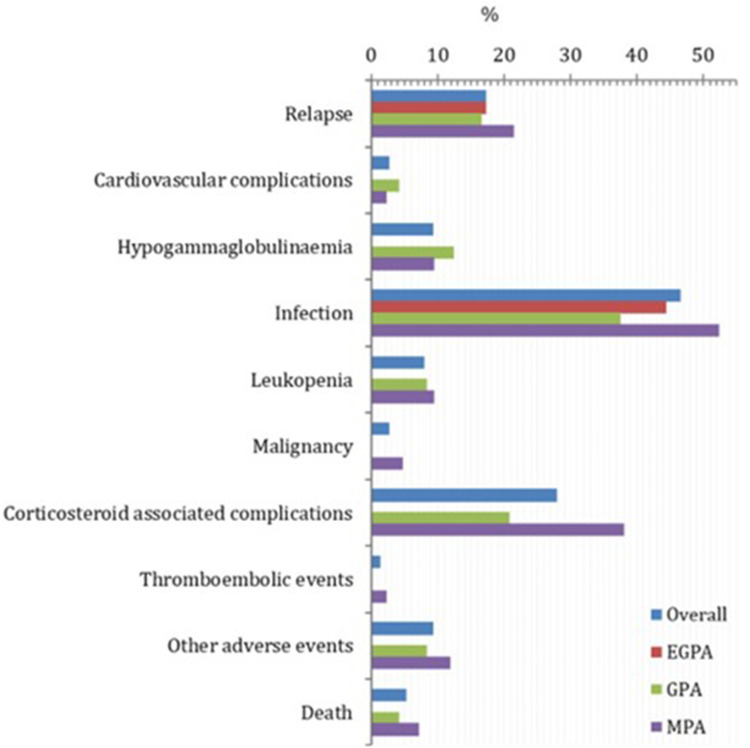
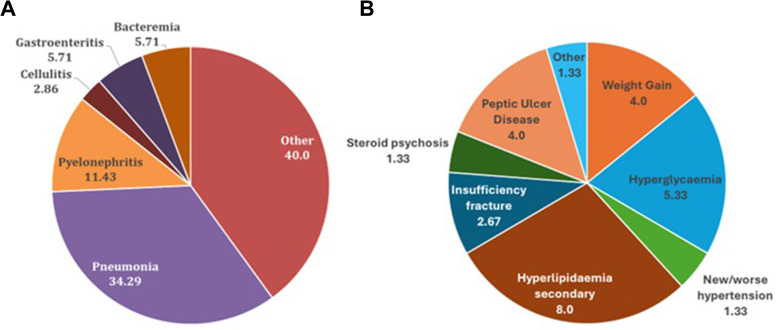
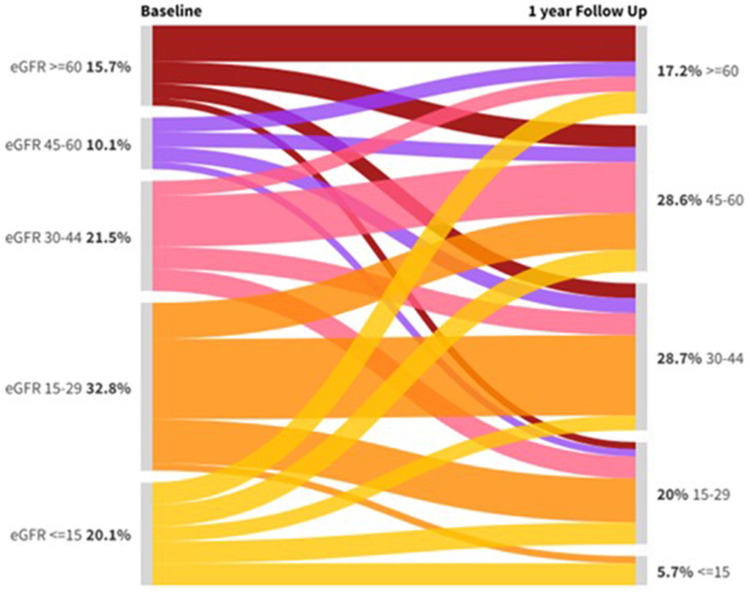
Results: Seventy-five patients (12% EGPA, 32% GPA, and 56% MPA) were included. Fifty-two percent were women. Mean age at diagnosis was 65.20±14.70 years. At baseline, mean BVAS was 17.35±5.70, 93.33% of patients showed renal affectation, mean estimated glomerular filtration rate was 33.32±29.93mL/min/1.73m2. As induction treatment, 62.67% received methylprednisolone, 37.33% rituximab, 25.33% cyclophosphamide, 14.67% rituximab plus cyclophosphamide, 34.67% plasmapheresis. During the first year after diagnosis, 17.33% relapsed and 78.67% had at least 1 hospitalisation; 97.33% received steroids; 13.33% were on dialysis at some point; one patient received a kidney transplant; 46.67% presented infections and 28% suffered corticosteroid-associated complications; 4 patients died, being 50% of deaths treatment-related. The highest observed mean cost per patient for the first year was €11,647.95 for hospital care.
Conclusion: This study revealed a considerable burden of AAV, as evidenced by high rates of hospitalisation, relapses, and the need for intensive medical interventions.
Keywords: anti-neutrophil cytoplasmic antibody-associated vasculitis; disease burden; registry; treatment outcome; vasculitis.
© 2025 Draibe et al.
Conflict of interest statement
ARA is an employee of CSL Vifor and may hold shares and/or stock options in the company. HDC, CC and JC are consultants of Axentiva Solutions, which received consultancy fees from CSL Vifor, Spain and, during the conduct of this study, from other pharmaceutical companies (Amgen, Pfizer, and Biogen) in unrelated projects. JD, FGP and LMV report having received a consulting fee from Axentiva Solutions for collaboration in this study and, during the conduct of this study, from other CSL Vifor-funded projects. The authors report no other conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
