

MRI ensemble model of plaque and perivascular adipose tissue as PET-equivalent for identifying carotid atherosclerotic inflammation
- PMID: 40768105
- PMCID: PMC12328859
- DOI: 10.1186/s13550-025-01293-9
MRI ensemble model of plaque and perivascular adipose tissue as PET-equivalent for identifying carotid atherosclerotic inflammation
Abstract
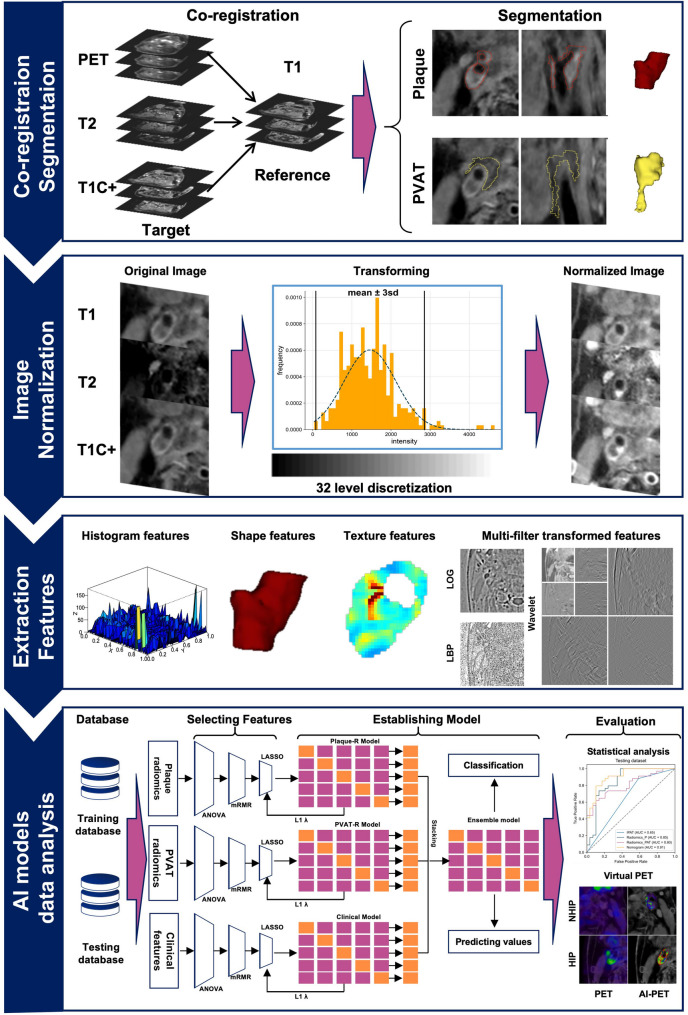
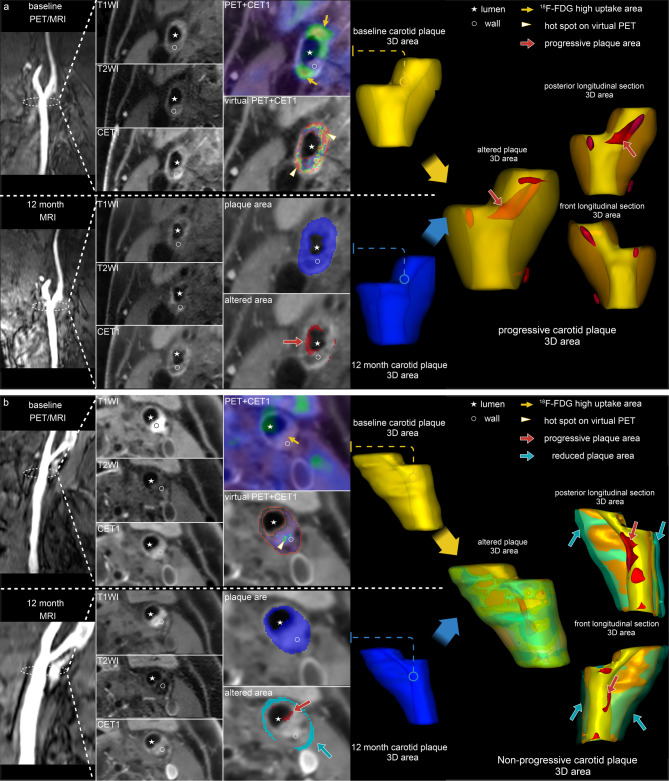
Background: Severe cerebrovascular events are associated with carotid atherosclerotic plaque progression and rupture that is mediated by inflammation. 18F-fluorodeoxyglucose ([18F]FDG) PET is important for assessing the inflammation of carotid atherosclerotic plaque, but it suffers from the limitations of radiation exposure. Additionally, inflammation of perivascular adipose tissue (PVAT) has been found to promote atherosclerosis progression through paracrine signaling mechanisms. The study aimed to develop an ensemble model based on carotid plaque and PVAT MRI radiomics for identifying highly inflammatory plaques (HIPs).
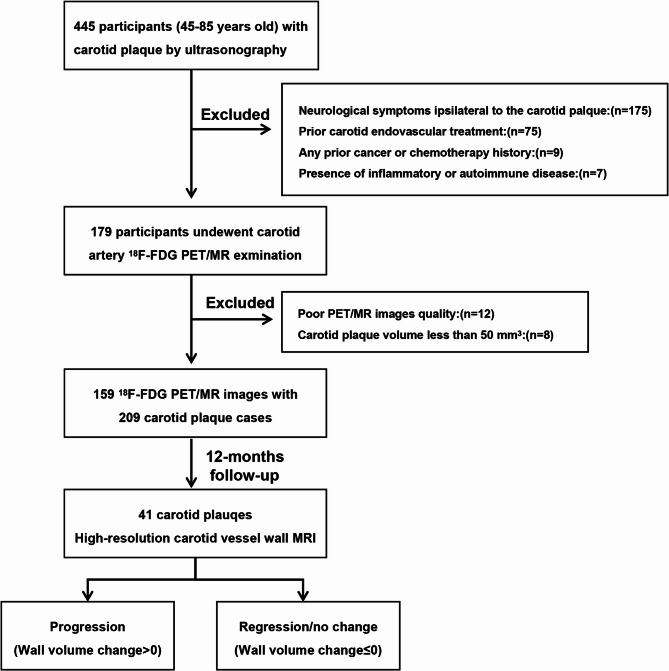
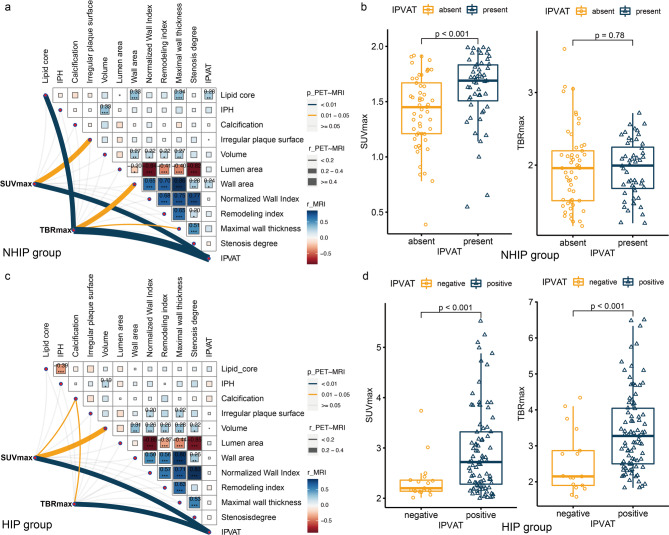
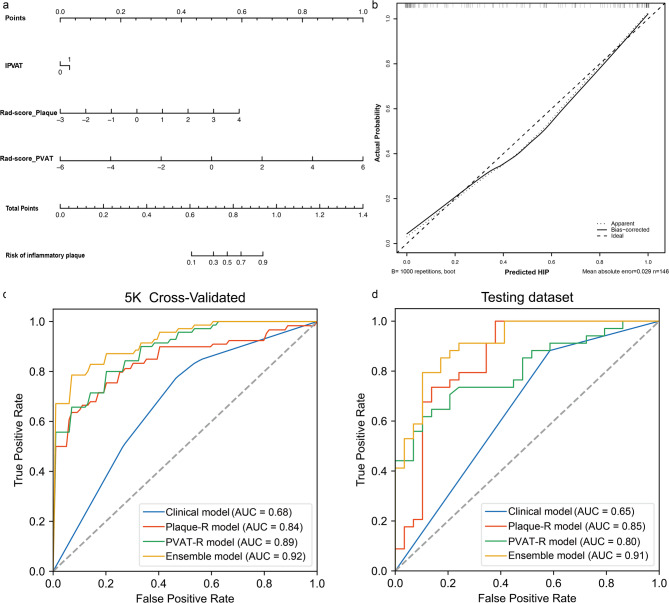
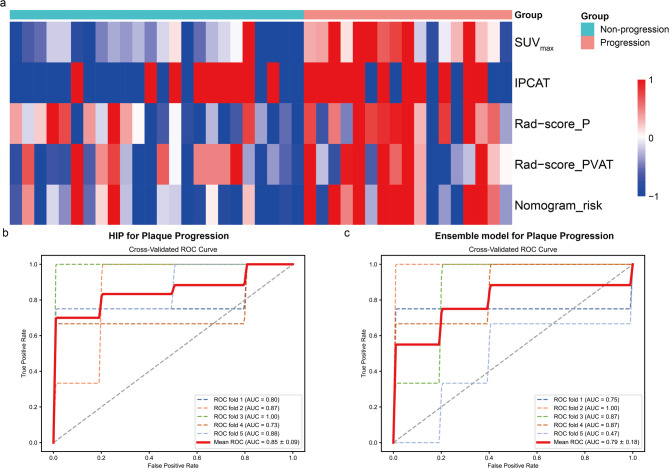
Results: 159 asymptomatic carotid atherosclerosis patients (137 males; 65 ± 8 years old) with 209 plaques (104 HIPs) were consecutively enrolled. 47.95% (70/146) of cases and 53.97% (34/63) were defined as HIPs in the training and testing datasets, respectively. There was more lipid core, more intraplaque hemorrhage, and less calcification in the HIPs compared to the non-highly inflammatory plaques (NHIPs) in the training dataset (p = 0.002, 0.019, and 0.013, respectively). Notably, the incidence of indistinct PVAT (IPVAT) in HIPs was higher than that in NHIPs, both in the training (81.43% vs. 46.05%; p < 0.001) and the testing (88.24% vs. 58.62%; p = 0.007) datasets. The correlations between plaque MRI characteristics and [18F]FDG uptake differed between the NHIPs and HIPs. However, IPVAT consistently correlated with SUVmax (r = 0.35, 0.30; p < 0.001, p = 0.002; for NHIPs and HIPs, respectively). The ensemble model that integrates the radiomics of carotid plaque and PVAT outperformed all models in predicting HIP (area under the curve [AUC] = 0.92/0.91, training/testing dataset). The follow-up further validated the PET for predicting plaque progression with the same accuracy as the ensemble model (AUC: 0.85 vs. 0.79).
Conclusions: The ensemble model integrating the radiomics of carotid plaque and perivascular adipose tissue provides an equivalent tool to PET in the visualization of the evaluation of carotid atherosclerosis inflammation and progression.
Keywords: Carotid atherosclerosis inflammation; PET/MRI; Perivascular adipose tissue; Radiomics.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This prospective cohort study was approved by the Xuanwu Hospital Medical Ethics Committee (No. LYS[2022]023). Written informed consent was obtained from all patients in this study. Consent for publication: The data presented have been approved for publication and each patient has provided written informed consent. Competing interests: The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures
Similar articles
-
Carotid Artery Surgery.2025 May 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 May 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 28722976 Free Books & Documents.
-
Development of a nomogram model using the dual-energy computed tomography angiography parameters of carotid plaque, the vascular lumen, and perivascular fat to predict acute stroke events.Quant Imaging Med Surg. 2025 Jun 6;15(6):4947-4959. doi: 10.21037/qims-2024-2765. Epub 2025 Jun 3. Quant Imaging Med Surg. 2025. PMID: 40606382 Free PMC article.
-
Predicting symptomatic carotid artery plaques with radiomics-based carotid perivascular adipose tissue characteristics: a multicenter, multiclassifier study.BMC Med Imaging. 2025 Aug 19;25(1):337. doi: 10.1186/s12880-025-01876-x. BMC Med Imaging. 2025. PMID: 40830841 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
References
-
- Vergallo R, Crea F. Atherosclerotic plaque healing. N Engl J Med. 2020;383(9):846–57. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
