

Acute aerobic exercise intensity does not modulate pain potentially due to differences in fitness levels and sex effects: results from a pharmacological fMRI study
- PMID: 40768346
- PMCID: PMC12327945
- DOI: 10.7554/eLife.102392
Acute aerobic exercise intensity does not modulate pain potentially due to differences in fitness levels and sex effects: results from a pharmacological fMRI study
Abstract
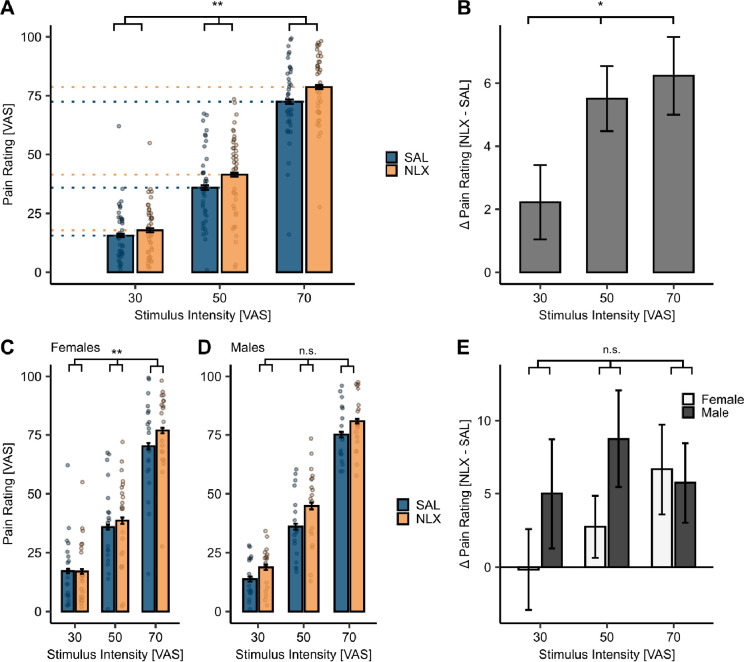
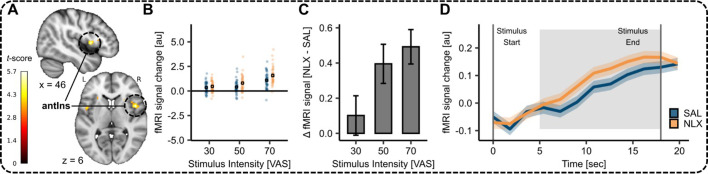
Exercise might lead to a release of endogenous opioids, potentially resulting in pain relief. However, the neurobiological underpinnings of this effect remain unclear. Using a pharmacological within-subject functional magnetic resonance imaging (fMRI) study with the opioid antagonist naloxone and different levels of aerobic exercise and pain, we investigated exercise-induced hypoalgesia (N = 39, 21 female). Overall, high-intensity (HI) aerobic exercise did not reduce pain as compared to low-intensity aerobic exercise. Accordingly, we observed no significant changes in the descending pain modulatory system. The µ-opioid antagonist naloxone significantly increased overall pain ratings but showed no interaction with exercise intensity. An exploratory analysis suggested an influence of fitness level (as indicated by the functional threshold power) and sex, where males showed greater hypoalgesia after HI exercise with increasing fitness levels. This effect was attenuated by naloxone and mirrored by fMRI signal changes in the medial frontal cortex, where activation also varied with fitness level and sex, and was reversed by naloxone. These results indicate that different aerobic exercise intensities have no differential effect on pain in a mixed population sample, but individual factors such as fitness level and sex might play a role. The current study underscores the need for personalised exercise interventions to enhance pain relief in healthy as well as chronic pain populations, taking into account the sex and fitness status as well as the necessity to further investigate the opioidergic involvement in exercise-induced pain modulation.
Keywords: exercise; human; hypoalgesia; medicine; naloxone; neuroimaging; neuroscience; opioids; pain.
Plain language summary
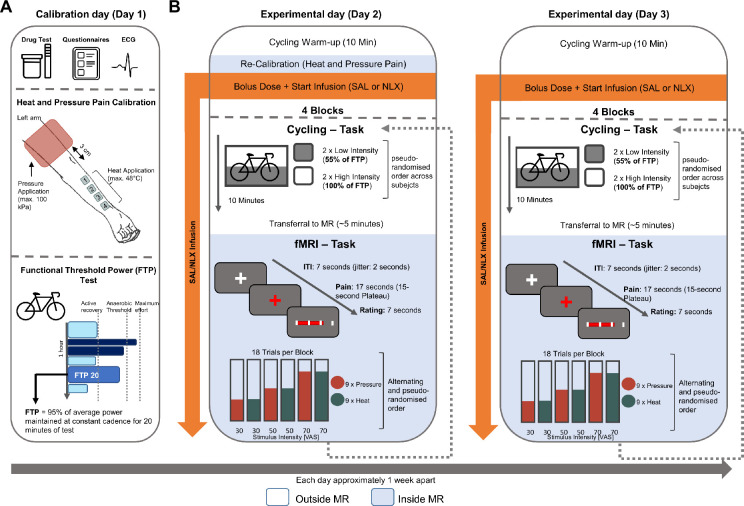
Many people turn to exercise as a way to relieve pain, hoping it will help them feel better. One reason this might work is because exercise can release natural chemicals in the body, called endogenous opioids, which help reduce pain. However, scientists still do not fully understand how this process works. Nold et al. explored how different levels of aerobic exercise – such as low vs. high intensity – affect how people feel pain. They used brain imaging and a medication called naloxone, which blocks the body’s opioid system, to better understand what is happening in the brain during exercise. The study included 39 healthy adults and looked at how factors like fitness level and sex might influence the effects of exercise on pain and how participants perceived pain. To determine whether high-intensity exercise provides more pain relief than low-intensity exercise, Nold et al. studied 18 males and 21 females during both high- and low-intensity exercises. Following the workout, magnetic resonance imaging was used to study brain activity as the participants received nine painful heat and pressure stimuli. Throughout the entire experiment, participants received a constant dose of either naloxone or a saline solution as a control. The study found that high-intensity exercise did not reduce pain any more than low-intensity exercise in the overall group. There were no major changes in how pain was processed in the brain and blocking the body’s opioids with naloxone made pain feel worse, regardless of how hard the participants exercised. However, more detailed analyses revealed that males with higher fitness levels experienced more pain relief after intense exercise than females. However, this effect disappeared when naloxone was given. Brain scans showed this was linked to activity in a part of the brain called the medial frontal cortex. These findings suggest that exercise may help reduce pain for some people more than others – especially depending on their sex and fitness level. In the future, personalized exercise programs could be developed to help manage pain more effectively. But before that can happen, more research is needed to understand exactly how the body’s natural pain-relief systems work during exercise, and how they differ between individuals.
© 2025, Nold et al.
Conflict of interest statement
JN, TF No competing interests declared, CB Senior editor, eLife
Figures



























Update of
- doi: 10.1101/2024.06.25.600579
- doi: 10.7554/eLife.102392.1
- doi: 10.7554/eLife.102392.2
Similar articles
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
Adapting Safety Plans for Autistic Adults with Involvement from the Autism Community.Autism Adulthood. 2025 May 28;7(3):293-302. doi: 10.1089/aut.2023.0124. eCollection 2025 Jun. Autism Adulthood. 2025. PMID: 40539213
-
Pain management for women in labour: an overview of systematic reviews.Cochrane Database Syst Rev. 2012 Mar 14;2012(3):CD009234. doi: 10.1002/14651858.CD009234.pub2. Cochrane Database Syst Rev. 2012. PMID: 22419342 Free PMC article.
-
Physical exercise training interventions for children and young adults during and after treatment for childhood cancer.Cochrane Database Syst Rev. 2016 Mar 31;3(3):CD008796. doi: 10.1002/14651858.CD008796.pub3. Cochrane Database Syst Rev. 2016. PMID: 27030386 Free PMC article.
References
-
- Allen H, Coggan A. Racing and Training with a Power Meter. Boulder, CO: VeloPress; 2006.
-
- Allen H, Coggan A. Training and Racing with a Power Meter. VeloPress; 2012.
-
- Årnes AP, Nielsen CS, Stubhaug A, Fjeld MK, Johansen A, Morseth B, Strand BH, Wilsgaard T, Steingrímsdóttir ÓA. Longitudinal relationships between habitual physical activity and pain tolerance in the general population. PLOS ONE. 2023;18:e0285041. doi: 10.1371/journal.pone.0285041. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
