

Application of mechanical quantitative techniques in postoperative rehabilitation assessment of anterior cruciate ligament reconstruction: A study protocol
- PMID: 40768443
- PMCID: PMC12327682
- DOI: 10.1371/journal.pone.0324663
Application of mechanical quantitative techniques in postoperative rehabilitation assessment of anterior cruciate ligament reconstruction: A study protocol
Abstract
This study protocol aims to explore the application of mechanical quantitative techniques in the postoperative rehabilitation assessment following anterior cruciate ligament reconstruction (ACLR). Anterior cruciate ligament injuries are prevalent among athletes and pose a considerable threat to their careers. While ACLR remains the primary therapeutic intervention for such injuries, the assessment of postoperative rehabilitation still encounters significant challenges. Traditional assessment methods are limited by subjectivity and the absence of quantitative data. Mechanical quantitative techniques present a novel approach, offering objective and precise quantitative metrics for knee functional rehabilitation through the analysis of soft tissue mechanical properties.
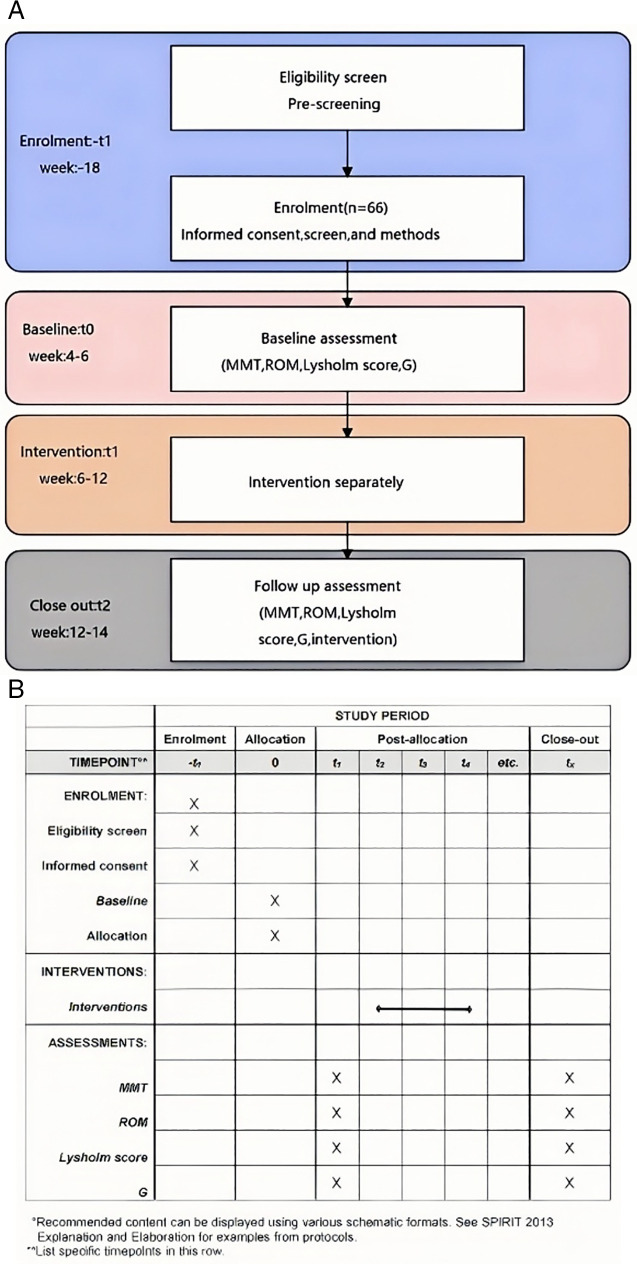
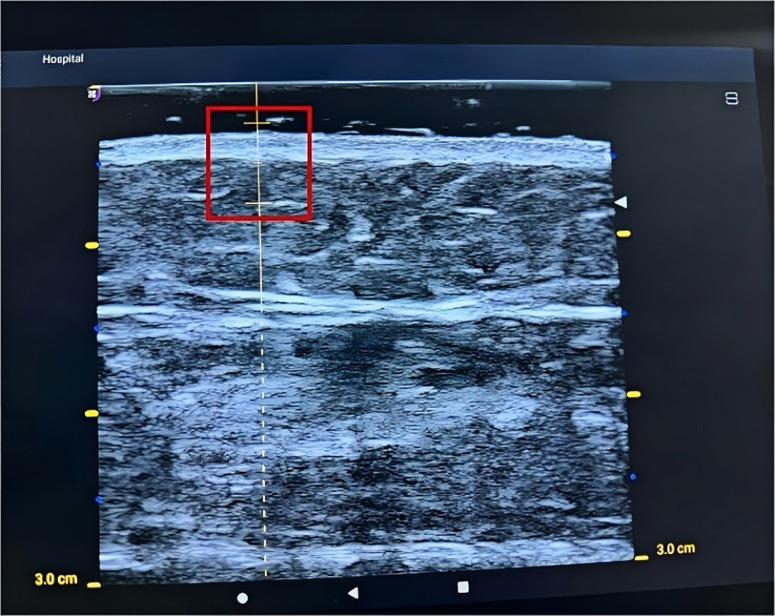
Methods: An observational methodology will be employed to gather clinical data from patients with ACL injuries. A soft tissue mechanical quantitative measurement device will be utilized for knee functional assessment. The anticipated sample size is 66 cases, with inclusion criteria encompassing specific age ranges, injury durations, and other pertinent factors. Exclusion criteria will exclude participants with other injuries or diseases that may impact rehabilitation. The assessment protocol will consist of traditional knee functional assessments, including knee muscle strength, range of motion, and Lysholm scores, as well as mechanical quantitative assessments of the quadriceps and hamstrings.
Blinding: Due to the inherent challenges in clinical controlled trials, a strict double-blind design is infeasible. Therefore, participants will be aware of their group assignments, whereas assessors will remain blinded to the specific research objectives and group allocations. Data entry and statistical grouping will be managed by independent personnel.
Statistical analysis: Data analysis is conducted using SPSS 20.0 software. Categorical data are represented as frequencies (percentages), with intergroup comparisons made using chi-square tests or exact probability methods; continuous data are represented as means ± standard deviations, with intergroup comparisons made using t-tests, analysis of variance, or rank sum tests, and correlation analysis is performed using Spearman's correlation coefficient. A P-value <0.05 is considered statistically significant.
Expected results: Firstly, It is anticipated that there will be a significant correlation between the assessment results of mechanical quantitative techniques and traditional functional assessment methods. This will validate the reliability of mechanical quantitative techniques and facilitate their complementary use alongside traditional assessment methods. Secondly. It is expected that this study will develop new scientific measurement tools and methods, mitigating errors associated with subjective judgments and ensuring the objectivity and accuracy of assessment results. By providing specific, quantifiable data, this study will offer physicians a more intuitive and precise basis for assessment.
Copyright: © 2025 Zhu et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Computer-assisted surgery for knee ligament reconstruction.Cochrane Database Syst Rev. 2014 Sep 3;2014(9):CD007601. doi: 10.1002/14651858.CD007601.pub4. Cochrane Database Syst Rev. 2014. PMID: 25180899 Free PMC article.
-
Computer-assisted surgery for knee ligament reconstruction.Cochrane Database Syst Rev. 2014 Aug 4;(8):CD007601. doi: 10.1002/14651858.CD007601.pub3. Cochrane Database Syst Rev. 2014. Update in: Cochrane Database Syst Rev. 2014 Sep 03;(9):CD007601. doi: 10.1002/14651858.CD007601.pub4. PMID: 25088229 Updated.
-
Surgical versus conservative interventions for treating anterior cruciate ligament injuries.Cochrane Database Syst Rev. 2016 Apr 3;4(4):CD011166. doi: 10.1002/14651858.CD011166.pub2. Cochrane Database Syst Rev. 2016. PMID: 27039329 Free PMC article.
-
The effects of contralateral limb cross-education training on post-surgical rehabilitation outcomes in patients with anterior cruciate ligament reconstruction: a randomized controlled trial.J Orthop Surg Res. 2025 Jan 30;20(1):118. doi: 10.1186/s13018-024-05430-3. J Orthop Surg Res. 2025. PMID: 39885535 Free PMC article. Clinical Trial.
-
One-incision versus two-incision techniques for arthroscopically assisted anterior cruciate ligament reconstruction in adults.Cochrane Database Syst Rev. 2017 Dec 15;12(12):CD010875. doi: 10.1002/14651858.CD010875.pub2. Cochrane Database Syst Rev. 2017. PMID: 29243827 Free PMC article.
References
-
- Feng J, Xu Y, Xu W. Advances in anterolateral ligament reconstruction: clinical practice and controversy. Chinese J Orthopaedics. 2023;43(5):328–36.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
