

Haemophilus influenzae in bronchiectasis
- PMID: 40769533
- PMCID: PMC12340525
- DOI: 10.1183/16000617.0007-2025
Haemophilus influenzae in bronchiectasis
Abstract
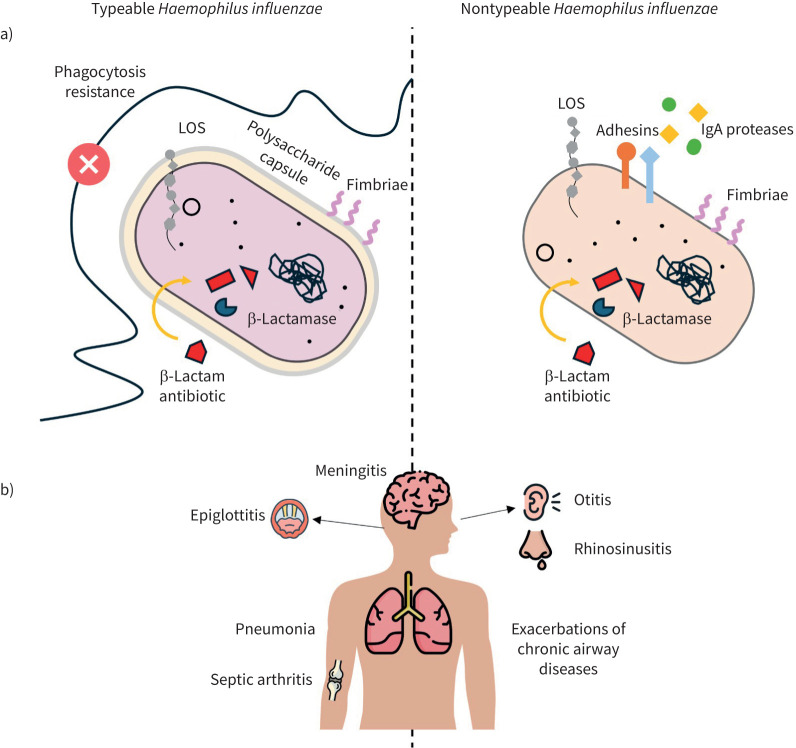
Bronchiectasis is a chronic respiratory disease characterised by irreversible bronchial dilation, persistent productive cough and alternating periods of clinical stability and exacerbations. The distorted airways impair mucus clearance, making them susceptible to recurrent infections and chronic inflammation. Haemophilus influenzae is a common pathogen in bronchiectasis according to international registries. It employs several virulence mechanisms, including adhesion, intracellular invasion/survival, biofilm formation and evasion of antibiotic treatments, to establish infection. These mechanisms allow H. influenzae to persist in the respiratory tract and evade host immune defences. Although its role is well-documented in other airway diseases, the impact of H. influenzae in bronchiectasis remains incompletely understood. International guidelines do not recommend eradication therapy for H. influenzae upon first isolation, while this intervention is advised for Pseudomonas aeruginosa in such cases. Long-term immunomodulatory treatment with macrolides is an option for patients with bronchiectasis with chronic H. influenzae infection and frequent exacerbations, though it carries the risk of promoting antibiotic resistance and a Pseudomonas-enriched airway microbiome. Studies indicate significant negative interactions between P. aeruginosa and H. influenzae, suggesting a competitive relationship that can influence microbiome dynamics and potentially affect clinical outcomes. Currently, there is insufficient evidence to support vaccination against nontypeable H. influenzae in chronic airways disease. Despite its frequent detection in respiratory samples, the precise role of H. influenzae in bronchiectasis-related morbidity and disease progression is not fully understood and warrants further investigation. This review examines the impact of H. influenzae on bronchiectasis pathophysiology and progression, comparing its role in other chronic respiratory diseases.
Copyright ©The authors 2025.
Conflict of interest statement
Conflict of interest: All authors declare that there is no relevant conflict of interest regarding the purpose of this review, as no suggestion or request from any organisation or company with potential vested interests influenced its conception.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical