

Selective lowest and upper instrumented vertebra for the correction of Lenke type 6C adolescent idiopathic scoliosis
- PMID: 40770047
- PMCID: PMC12329009
- DOI: 10.1038/s41598-025-14783-6
Selective lowest and upper instrumented vertebra for the correction of Lenke type 6C adolescent idiopathic scoliosis
Abstract
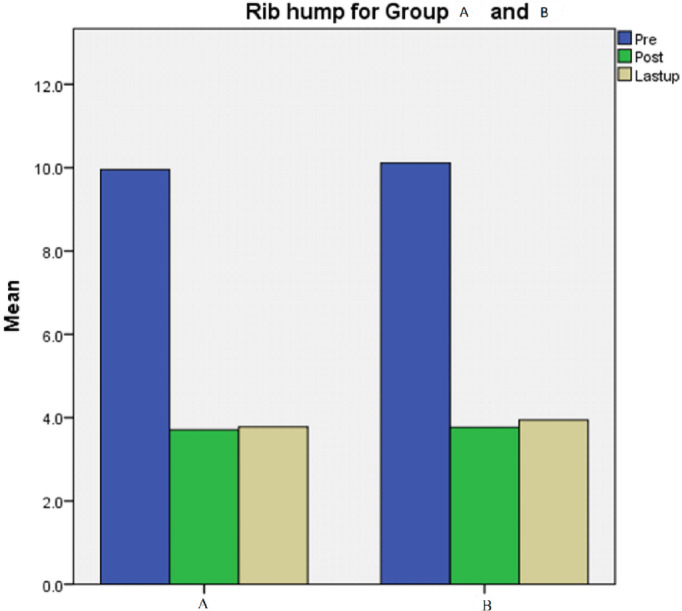
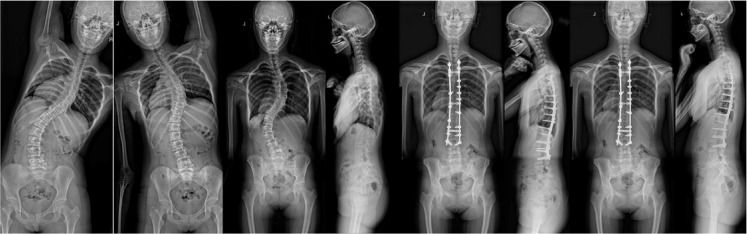
Retrospective Study. The selection of the upper instrumented vertebra (UIV) and lowest instrumented vertebra (LIV) in adolescent idiopathic scoliosis (AIS) Lenke type 6C is critical for achieving optimal spinal alignment and preventing post-surgical complications. This study evaluates the radiographic and clinical outcomes of two UIV and LIV selection strategies in patients with AIS Lenke 6C undergoing posterior spinal fusion. A retrospective analysis was conducted on 79 patients treated between 2011 and 2020. Patients were divided into two groups based on LIV and UIV selection: Group A, with LIV at the lower end vertebra (LEV) and UIV at the upper end vertebra (UEV), and Group B, with LIV one level caudal to the LEV (LEV-1) and UIV either one level above or below the UEV (UEV + 1 or UEV-1). Radiographic parameters, including coronal and sagittal balance, and clinical outcomes were compared between the groups. Both groups demonstrated significant improvements in spinal alignment. In Group A, the thoracic and lumbar/thoracolumbar Cobb angles improved from 36.1 ± 6° and 51.3 ± 3° preoperatively to 1.8 ± 0° and 2.8 ± 1° at six months postoperatively, and 1.7 ± 0° and 3.1 ± 2° at the final follow-up. In Group B, the thoracic and lumbar/thoracolumbar Cobb angles improved from 33.6 ± 5° and 51.7 ± 3° preoperatively to 2.6 ± 2° and 3.7 ± 2° at six months postoperatively, and 2.6 ± 2° and 3.7 ± 2° at the final follow-up (P = 0.105). Coronal and sagittal balance parameters showed comparable improvements in both groups. The SRS-22 scores at the final follow-up indicated significant enhancements in all domains, including pain, function, and mental well-being. The selection of UIV and LIV significantly impacts radiographic and clinical outcomes in AIS Lenke type 6C. Both strategies-LIV at LEV with UIV at UEV, and LIV at LEV-1 with UIV at UEV ± 1yielded comparable improvements in spinal alignment and patient-reported outcomes. However, the choice of UIV and LIV should be tailored to individual patient anatomy and surgical goals. This study underscores the importance of careful UIV and LIV selection in optimizing postoperative outcomes for AIS Lenke type 6C patients.
Keywords: AIS; Fusion; Lenke 6C; Posterior only; Selective.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests. Ethical statement: All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and approve this version to be published. The ethical committee of Xiangya Hospital, Central South University approved the study, and informed consent was obtained from all subjects and/or legal guardian(s). Furthermore, all methods were performed per our hospital’s relevant guidelines and regulations. Ethics approval number 21017033559.
Figures

References
-
- Karol, L. A., Virostek, D., Felton, K., Jo, C. & Butler, L. The Effect of the Risser Stage on Bracing Outcome in Adolescent Idiopathic Scoliosis Journal of Bone and Joint Surgery 98(15), 1253–1259 (2016). - PubMed
-
- Yanik, H. S., Ketenci, I. E. & Erdem, S. Lowest instrumented vertebrae selection in posterior fusion of Lenke 3 C/6 C adolescent idiopathic scoliosis: L3 versus L4, when LEV is L4. Arch Orthop Trauma Surg [Internet]. 2023;(0123456789). Available from: 10.1007/s00402-023-04872-4 - PubMed
-
- Li, J. et al. Selective Fusion in Lenke 5 Adolescent Idiopathic Scoliosis. World Neurosurg [Internet]. ;118:e784–91. (2018). Available from: 10.1016/j.wneu.2018.07.052 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
