

A novel chimeric antigen receptor T-cell therapy targeting CD84 for the treatment of acute myeloid and T-cell lymphoblastic leukemias
- PMID: 40770072
- PMCID: PMC12463657
- DOI: 10.1038/s41375-025-02705-4
A novel chimeric antigen receptor T-cell therapy targeting CD84 for the treatment of acute myeloid and T-cell lymphoblastic leukemias
Abstract
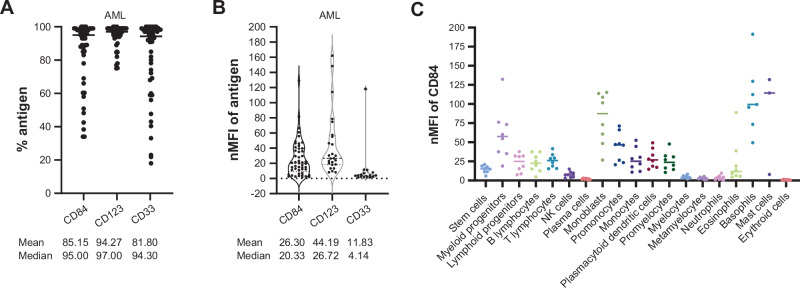
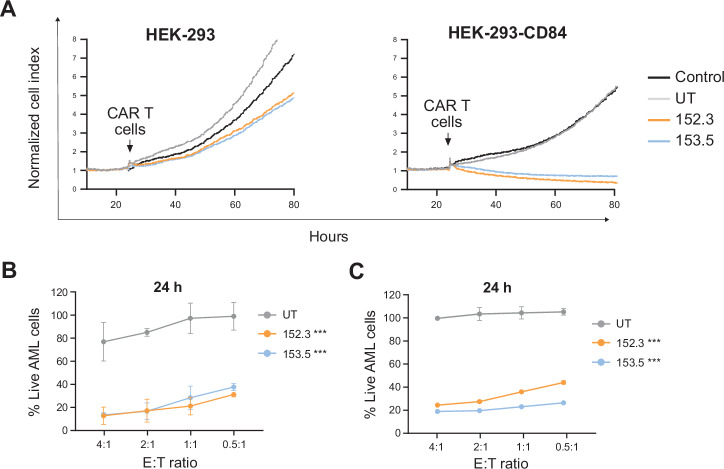
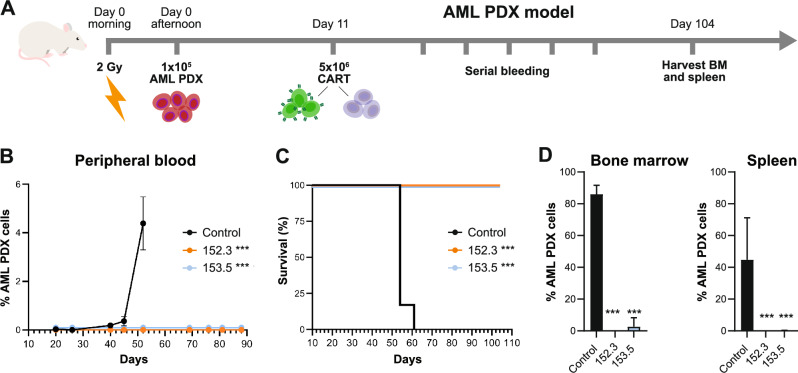
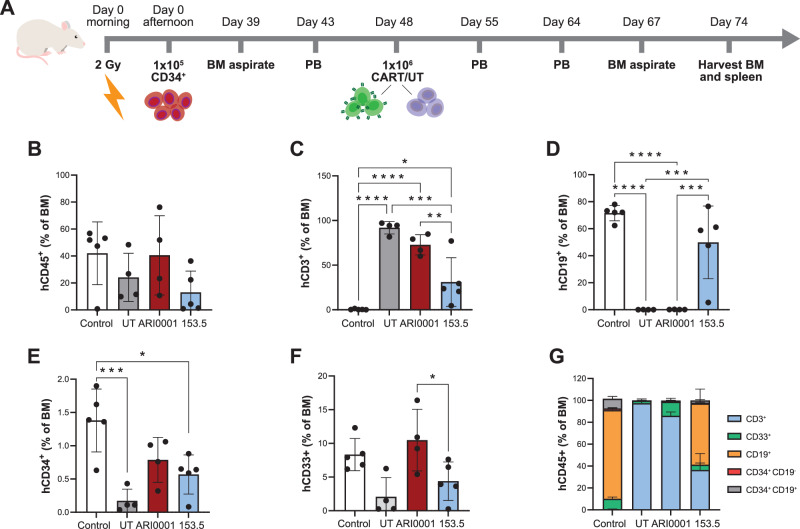
Despite the remarkable clinical successes of chimeric antigen receptor (CAR) T-cell therapies in treating B-cell malignancies and multiple myeloma, similar outcomes have not been achieved in other indications. For patients with relapsed or refractory (R/R) acute myeloid leukemia (AML) or T-cell acute lymphoblastic leukemia (T-ALL), treatment options are limited, yet CART-cell therapies offer significant potential to address this unmet need. Here, we introduce a first-in-class CART-cell therapy targeting CD84, a novel antigen, for the treatment of R/R AML and T-ALL. CD84 is highly expressed on leukemic blasts, with limited expression on hematopoietic stem progenitor cells (HSPC), and is largely absent in healthy human tissues. Our second-generation CARTs targeting CD84 (CART84) demonstrate potent cytotoxicity against AML and T-ALL cells both in vitro and in vivo in patient-derived xenograft (PDX) models. Furthermore, CART84 eliminated primary leukemic blasts while exhibiting low cytotoxicity against CD34+ HSPC in vitro and in humanized mouse models in vivo, suggesting a low risk of myelotoxicity. These results support CD84 as a promising target for AML and T-ALL and provide the foundation for our upcoming first-in-human phase I/II clinical trial using CD84-directed CAR T cell therapy for patients with R/R AML and T-ALL (EudraCT 2024-519966-31-00).
© 2025. The Author(s).
Conflict of interest statement
Competing interests: PM is a cofounder of OneChain ImmunoTx, a spin-off company unrelated to this work. LP, MAU, SP, and NKG are employees of Gyala Therapeutics S.L., NKG is partially employed by Gyala Therapeutics S.L., a spin-off company of the Hospital Clínic of Barcelona related to this work. CS is the CEO of Gyala Therapeutics S.L., a spin-off company related to this work. LP, CS, MJ, and NKG declare to be co-inventors in the patent of PCT/EP2023/050194. MJ declares Research Funding from Gyala Therapeutics S.L. Ethics approval and consent to participate: All methods were performed in accordance with the relevant guidelines and regulations, including the Declaration of Helsinki. Approval for the use of human samples was obtained from the Clinical Research Ethics Committee of Hospital Clínic of Barcelona, under protocol numbers HCB/2021/0977 and HCB/2016/0045. Informed consent was obtained from all participants or their legal guardians prior to sample collection (reference code R121004-094). Approval for experiments involving animals was obtained from the Animal Experimentation Ethics Committee of Generalitat de Catalunya, under protocol number 11577.
Figures



References
-
- Hong M, Clubb JD, Chen YY. Engineering CAR-T cells for next-generation cancer therapy. Cancer Cell. 2020;38:473–88. - PubMed
-
- Abramson JS, Palomba ML, Gordon LI, Lunning MA, Wang M, Arnason J, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study. Lancet. 2020;396:839–52. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
