

Single-cell atlas reveals heterogeneous response to FcRn blockade in anti-AChR antibody-positive generalised myasthenia gravis
- PMID: 40770830
- PMCID: PMC12328247
- DOI: 10.1002/ctm2.70436
Single-cell atlas reveals heterogeneous response to FcRn blockade in anti-AChR antibody-positive generalised myasthenia gravis
Abstract
Background: Myasthenia gravis (MG) is an autoimmune disease predominantly driven by autoantibodies targeting acetylcholine receptor (AChR), resulting in muscle weakness. Efgartigimod, a neonatal Fc receptor (FcRn) blocker, reduces pathogenic immunoglobulin G in anti-AChR antibody-positive generalised MG (gMG). This study aimed to identify immune mechanisms underlying MG pathology and response to efgartigimod.
Methods: We constructed a single-cell atlas of peripheral immune cells from treatment-naïve and efgartigimod-treated patients with gMG. Comprehensive immunophenotyping was performed to compare the clonal diversity of B- and T-cell populations, alongside experimental validation to assess the activation of Th17-related pathways before and after FcRn blockade.
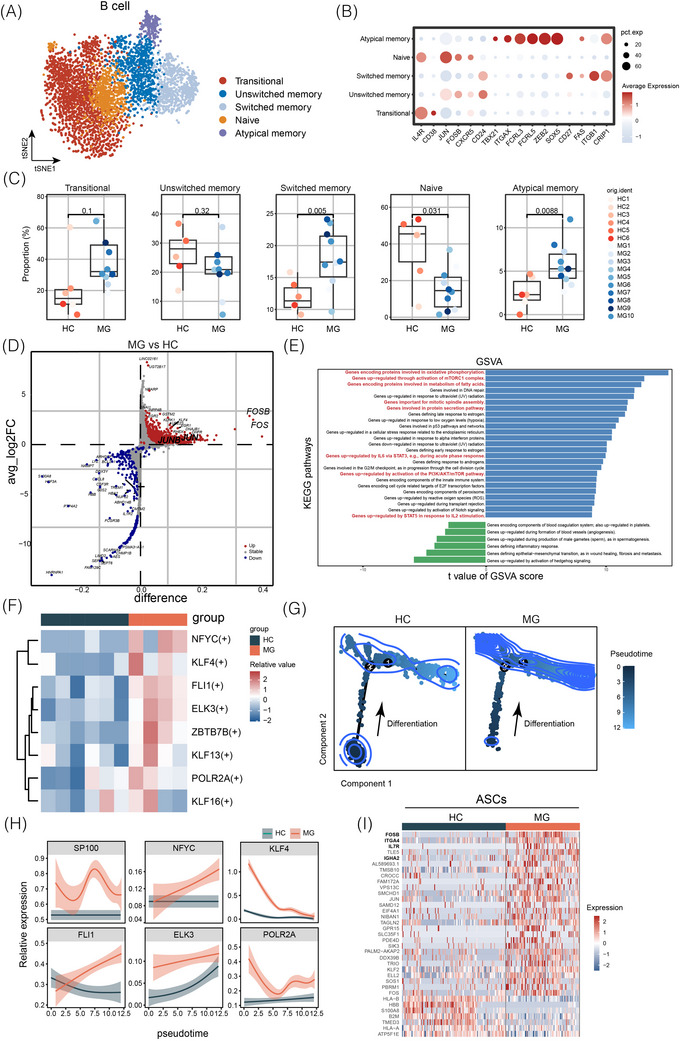
Results: B cells in patients with gMG exhibit heightened activation and differentiation, while T cells display distinct pro-inflammatory phenotypes. Enhanced intercellular signalling contributed to the pathogenicity associated with gMG. Efgartigimod mitigated upregulated antigen processing and presentation pathways in MG. Additionally, B-cell clonal diversity and IGHG1-bearing B-cell receptors increased. Transcriptional factor alterations were noted in suboptimal responders. Regulation of T-cell activity, particularly within Th17-related pathways, was associated with remission rates.
Conclusions: These findings underscore immune heterogeneity and dynamics during efgartigimod treatment, providing mechanistic insights into therapeutic response in gMG.
Key points: Aberrant B cells and pro-inflammatory T cells contribute critically to generalised myasthenia gravis (gMG) pathogenesis. Neonatal Fc receptor (FcRn) blockade induces immunoglobulin G (IgG) depletion feedback, reflected by increased class-switched BCRs. Th17 cell proliferation is attenuated following FcRn blockade. Antigen processing and presentation pathways are downregulated after FcRn blockade in gMG.
Keywords: FcRn blockade; myasthenia gravis; single‐cell RNA sequencing; therapeutic response.
© 2025 The Author(s). Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
The authors declare they have no conflicts of interest.
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous