

Real-world patterns of immunoglobulin replacement therapy for infection prevention in common variable immunodeficiency: a multicenter nationwide study
- PMID: 40771807
- PMCID: PMC12325207
- DOI: 10.3389/fimmu.2025.1640290
Real-world patterns of immunoglobulin replacement therapy for infection prevention in common variable immunodeficiency: a multicenter nationwide study
Abstract
Background and aims: Immunoglobulin replacement therapy (IgRT), administered intravenously (IVIg) or subcutaneously (SCIg), is the cornerstone treatment for patients with Common Variable Immunodeficiency (CVID). Although both modalities demonstrate similar efficacy, SCIg is associated with fewer systemic adverse events and increased patient autonomy. Despite these advantages, its utilization remains limited in certain regions, particularly in the Mediterranean region. This study aimed to evaluate real-world patterns of IgRT use in Spanish CVID patients and provide a comprehensive analysis of the factors associated with IVIg and SCIg administration in routine clinical practice.
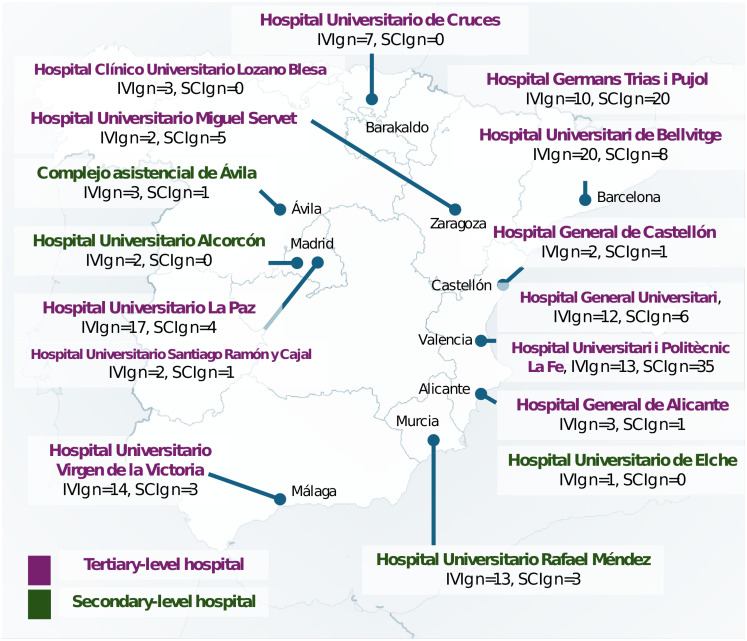
Methods: A cross-sectional, multicenter study was conducted using data from the GTEM-SEMI-CVID Registry, encompassing 212 adult CVID patients receiving IgRT across Spain. Patients were grouped based on the administration route: IVIg and SCIg. Demographic, clinical, and immunological data, including IgRT modality, dosage, administration setting, and comorbidities, were collected. Comparative statistical analyses were performed to identify differences between both treatment groups.
Results: Of the 212 patients, 58.5% received IVIg and 41.5% received SCIg. SCIg recipients were younger (47.5 vs. 54.8 years, p = 0.003) and predominantly treated at home (80.6% vs. 1.6%, p < 0.001), compared to those receiving IVIg. SCIg use was significantly higher in tertiary hospitals compared to secondary ones (44.4% vs. 17.4%, p = 0.0136). Infection rates, autoimmune comorbidities, weekly doses (7.2 g for IVIg vs. 7.7 g for SCIg, p = 0.142), and IgG trough levels were comparable across groups.
Conclusion: This study provides real-world evidence on IgRT patterns in Spanish patients with CVID, revealing a marked increase in SCIg use over the past decade, although IVIg remains predominant, especially in secondary hospitals. Age significantly influenced the choice of modality, with IVIg preferred for older patients and SCIg for younger ones, while disease severity did not impact this decision. These findings underscore the need to optimize access to SCIg, particularly in secondary centers, to enhance patient autonomy and improve therapeutic outcomes.
Keywords: common variable immunodeficiency (CVID); immunoglobulin replacement therapy (IGRT); intravenous immunoglobulin (IVIg); real-world evidence; subcutaneous immunoglobulin (SCIg).
Copyright © 2025 Moral Moral, Garcia-Bustos, Balastegui-Martin, Martínez Mercader, Bracke, Mateu, Solanich, Antolí, Carrillo-Linares, Robles-Marhuenda, Puchades, Pelaez Ballesta, López-Osle, Torralba-Cabeza, Bielsa Masdeu, Gil Niño, Tornador Gaya, Pascual Castellanos, Sánchez-Martínez, Barragán-Casas, González-García, Patier de la Peña, López-Wolf, Mora Rufete, Canovas Mora and Cabañero-Navalon.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Orange JS, Hossny EM, Weiler CR, Ballow M, Berger M, Bonilla FA, et al. Use of intravenous immunoglobulin in human disease: a review of evidence by members of the Primary Immunodeficiency Committee of the American Academy of Allergy, Asthma and Immunology. J Allergy Clin Immunol. (2006) 117:S525–53. doi: 10.1016/j.jaci.2006.01.015, PMID: - DOI - PubMed
-
- Abolhassani H, Sadaghiani MS, Aghamohammadi A, Ochs HD, Rezaei N. Home-based subcutaneous immunoglobulin versus hospital-based intravenous immunoglobulin in treatment of primary antibody deficiencies: systematic review and meta analysis. J Clin Immunol. (2012) 32:1180–92. doi: 10.1007/s10875-012-9720-1, PMID: - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous