

Neuropsychiatric symptoms cluster as primary drivers of Long COVID complexity: a South Texas retrospective cohort study
- PMID: 40771985
- PMCID: PMC12325076
- DOI: 10.3389/fneur.2025.1612489
Neuropsychiatric symptoms cluster as primary drivers of Long COVID complexity: a South Texas retrospective cohort study
Abstract
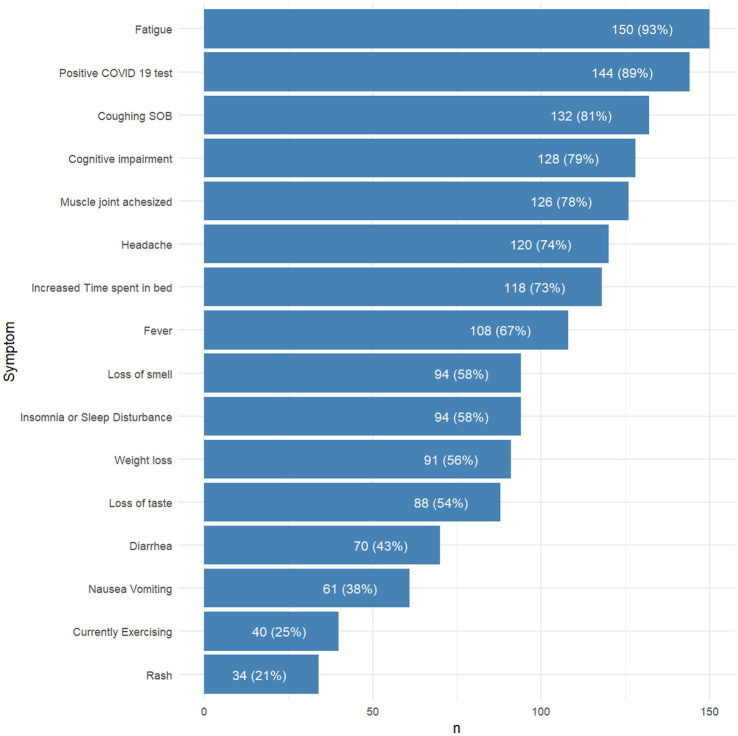
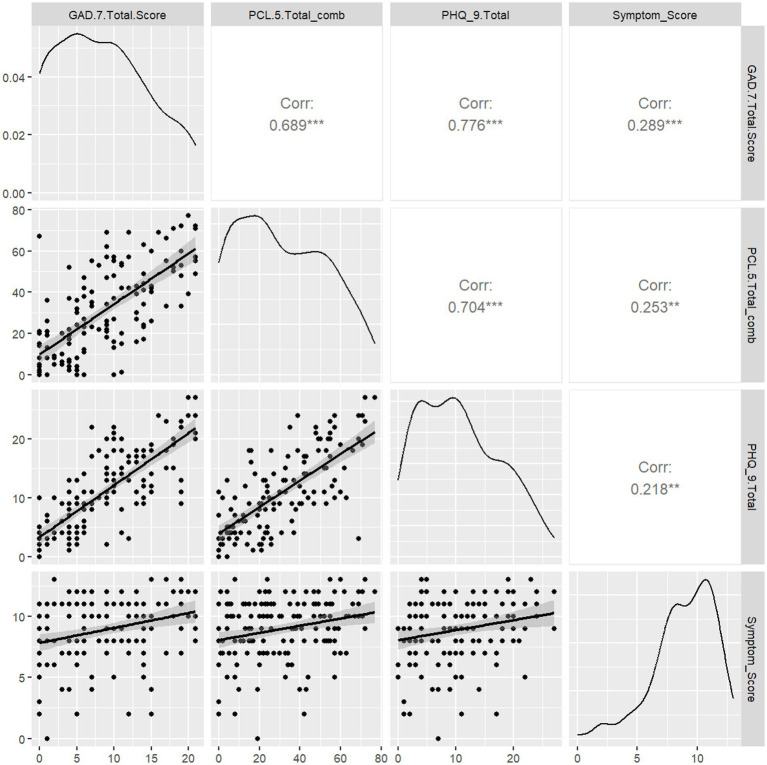
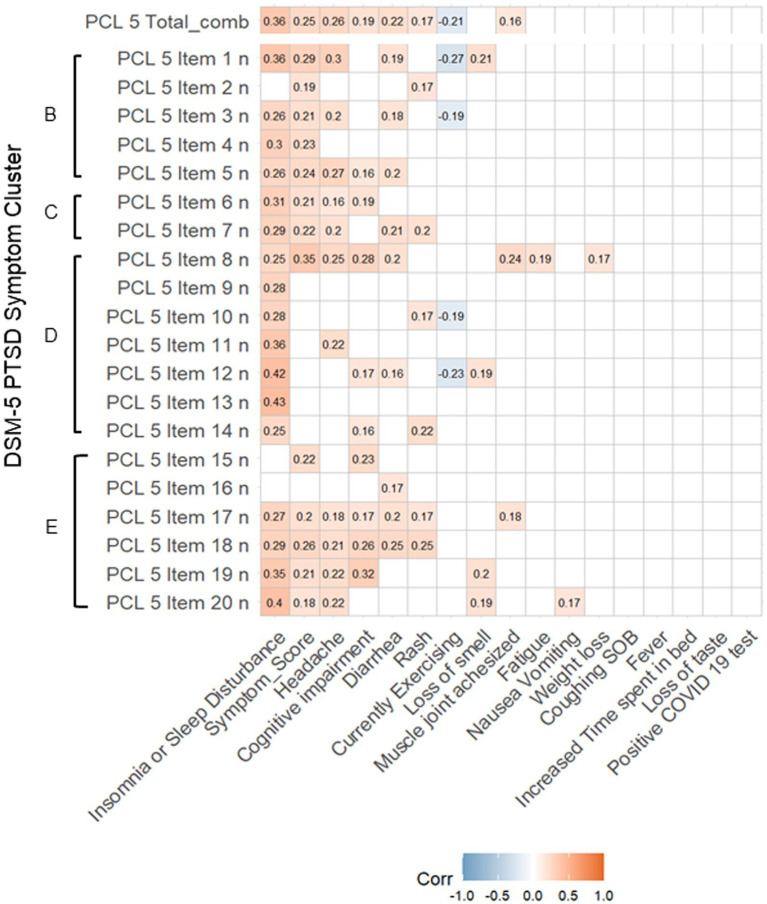
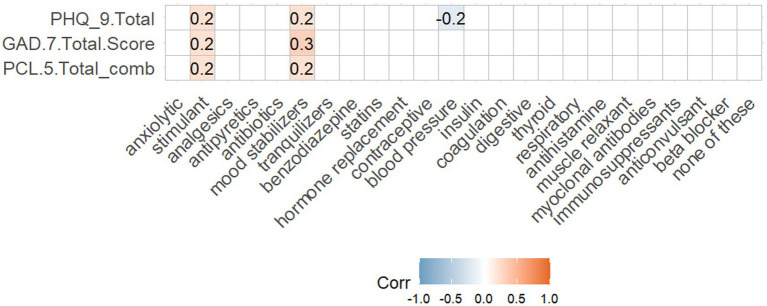
Long COVID, previously known as Post-Acute Sequelae of SARS-CoV-2 (PASC), refers to prolonged symptoms or diagnosable conditions following COVID-19 infection. The neuropsychiatric profile of Long COVID patients remains ambiguous. This study aimed to assess neuropsychiatric symptoms in a retrospective cohort of Long COVID patients (N = 162) at a Rehabilitation Medicine clinic in South Texas. Clinical data from patient records were used to calculate a Symptom Score, and screening tools for stress/PTSD (PCL-5), depression (PHQ-9), anxiety (GAD-7), and quality of life (SWL) were employed to evaluate if Long COVID duration and severity could predict neuropsychiatric outcomes. The majority were female (71%) and Hispanics (53%) who presented for treatment of Long COVID symptoms during the study period, including fatigue (93%), coughing/shortness of breath (81%), fever (67%), anosmia (58%), ageusia (54%), and weight loss (56%). A minority of participants were hospitalized (N = 49) or required ventilator support (N = 5) during acute infection. There was a high burden of neuropsychiatric symptoms, including subjective cognitive impairment (79%), headache (74%), and insomnia (58%). Symptom Score (median = 9, IQR [8,11]) was significantly correlated with increased depression (PHQ-9; p < 0.05), anxiety (GAD-7; p < 0.05) and elevated stress/PTSD (PCL-5; p < 0.05) symptoms. Long COVID patients taking stimulants or mood stabilizers had higher GAD-7 (p < 0.031, p < 0.035) and PHQ-9 (p < 0.034, p < 0.009) scores but not PCL-5 scores. Importantly, duration of Long COVID symptomatology also did not predict PCL-5 scores. No patient factors (e.g., sex, age, BMI, ethnicity) mediated Symptom Score. Nonetheless, historically marginalized groups, such as women and Hispanics, have been disproportionately affected by COVID-19. This study is the first to utilize validated screening tools to determine the presence and severity of neuropsychiatric symptoms in Long COVID patients. These findings may guide clinical management and future research on Long COVID, especially in historically excluded populations.
Keywords: GAD-7; Long COVID; PCL-5; PHQ-9; PTSD; anxiety; depression; stress.
Copyright © 2025 Wells, Rolin, Robles-Ramamurthy, Gibson-Lopez, Goros, Gelfond, Gelfond, Balfanz, Deuter, McGeary and Verduzco-Gutierrez.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Update of
-
Assessing Neuropsychiatric Symptoms in Long COVID: A Retrospective Cohort Study from a South Texas Long COVID Clinic.medRxiv [Preprint]. 2025 Jun 16:2024.11.03.24316669. doi: 10.1101/2024.11.03.24316669. medRxiv. 2025. Update in: Front Neurol. 2025 Jul 23;16:1612489. doi: 10.3389/fneur.2025.1612489. PMID: 40585077 Free PMC article. Updated. Preprint.
References
-
- WHO . Director-general’s opening remarks at the media briefing. (2023). Available online at: https://www.who.int/director-general/speeches/detail/who-director-genera... (Accessed May 05, 2023).
-
- Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. Features, evaluation, and treatment of coronavirus (COVID-19) In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; (2023) - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous