

Towards a universal implementation of labor companionship: a synthesis of the policy and facility environment of eight low-and-middle income countries
- PMID: 40772012
- PMCID: PMC12325283
- DOI: 10.3389/frhs.2025.1550473
Towards a universal implementation of labor companionship: a synthesis of the policy and facility environment of eight low-and-middle income countries
Abstract
Background: Labor companionship, the presence of a woman's person of choice during childbirth, has benefits to both woman and baby and is recommended by the World Health Organization since 2012. However, implementation remains sub-optimal, especially in low-and-middle-income countries (LMICs). This study aimed to understand the maturity of labor companionship implementation in eight low-and-middle income countries with focus on the policy and facility environment.
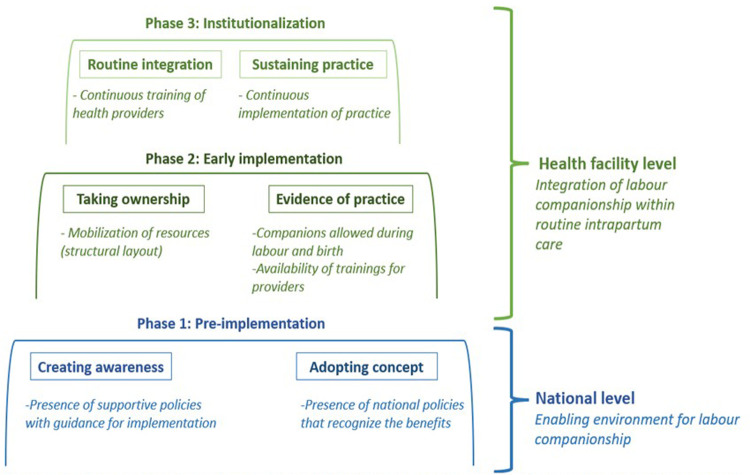
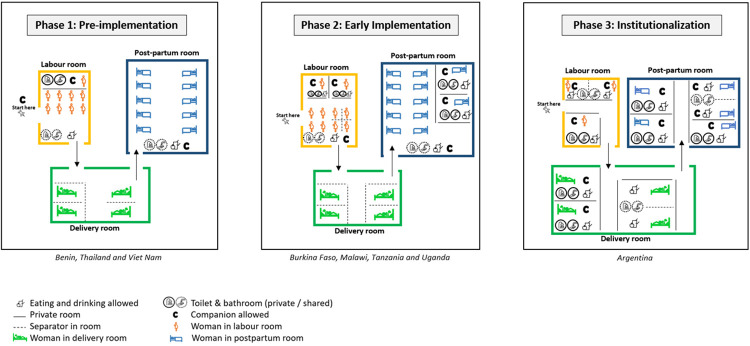
Methods: This was a multi-country study nested in two hospital-based implementation research studies: Action Leveraging Evidence to Reduce perinatal mortality and morbidity in Sub-Saharan Africa (ALERT) study and the QUALIty DECision-making by women and providers for appropriate use of caesarean section (QUALI-DEC) study. We included 48 hospitals from eight countries: Argentina, Burkina Faso, Thailand and Viet Nam (QUALI-DEC) and four from each of Benin, Malawi, Tanzania and Uganda (ALERT). We used data from (i) a document review, including national policy documents and (ii) health facility readiness assessment, including physical layouts of maternity wards, all collected between December 2019 and April 2021. Our analysis included two steps, (1) a structured data abstraction with coding to pre-defined categories to analyse the national polices and available resources on a facility level which informed the (2) categorization of implementation maturity in three implementation phases modelled by the framework by Bergh et al. and the logic model developed by Bohren et al.
Results: Three of the eight countries lacked any national-level companionship policies, four had some mentioning and only one had detailed guidance on roles of labor companions and implementation guidelines. The physical outlines of maternity wards varied greatly, and lack of space was one of the main implementation barriers to all countries except Argentina. We classified Benin, Thailand and Viet Nam in the pre-implementation phase because of missing guidelines and limited implementation; Burkina Faso, Malawi, Uganda and Tanzania in the early implementation phase; and Argentina in the institutionalization phase where policies and facility resources were conducive.
Conclusion: Successful implementation was supported by concrete and contextualized implementation guidance. To move to high implementation levels, supporting policies, guidelines and structural changes in the maternity wards are needed.
Keywords: LMICs; childbirth; health policy; implementation research; intrapartum care; labor companionship; maternal health; quality of care.
© 2025 El-Halabi, Pembe, Dumont, Betrán, Kaboré, Chipeta, Carroli, Alvesson, Kidanto, Dossou, Annerstedt, Beňová, Gross, Waiswa, Lumbiganon, Mac, Bohren and Hanson.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Planning for scale: analysis of adaptations and contextual factors influencing scale-up of the QUALI-DEC intervention to optimize caesarean section use.Implement Sci Commun. 2025 May 21;6(1):61. doi: 10.1186/s43058-025-00737-6. Implement Sci Commun. 2025. PMID: 40400046 Free PMC article.
-
Factors that influence the provision of intrapartum and postnatal care by skilled birth attendants in low- and middle-income countries: a qualitative evidence synthesis.Cochrane Database Syst Rev. 2017 Nov 17;11(11):CD011558. doi: 10.1002/14651858.CD011558.pub2. Cochrane Database Syst Rev. 2017. PMID: 29148566 Free PMC article.
-
[Volume and health outcomes: evidence from systematic reviews and from evaluation of Italian hospital data].Epidemiol Prev. 2013 Mar-Jun;37(2-3 Suppl 2):1-100. Epidemiol Prev. 2013. PMID: 23851286 Italian.
-
Consumers' and health providers' views and perceptions of partnering to improve health services design, delivery and evaluation: a co-produced qualitative evidence synthesis.Cochrane Database Syst Rev. 2023 Mar 14;3(3):CD013274. doi: 10.1002/14651858.CD013274.pub2. Cochrane Database Syst Rev. 2023. PMID: 36917094 Free PMC article.
-
Planned early delivery versus expectant management for hypertensive disorders from 34 weeks gestation to term.Cochrane Database Syst Rev. 2017 Jan 15;1(1):CD009273. doi: 10.1002/14651858.CD009273.pub2. Cochrane Database Syst Rev. 2017. PMID: 28106904 Free PMC article.
References
-
- World Health Organization. WHO Recommendations on Intrapartum Care for a Positive Childbirth Experience. Geneva: World Health Organization; (2018). p. 210. Available online at: https://www.who.int/publications/i/item/9789241550215 (Accessed January 1, 2023). - PubMed
-
- WHO. Standards for Improving Quality of Maternal and Newborn Care in Health Facilities. Geneva: World Health Organization; (2016). p. 84. Available online at: https://cdn.who.int/media/docs/default-source/mca-documents/advisory-gro... (Accessed January 1, 2023).
-
- WHO. WHO Recommendations for Augmentation of Labour. Geneva: World Health Organization; (2014). Available online at: https://apps.who.int/iris/bitstream/handle/10665/112825/9789241507363_en... (Accessed January 1, 2023). - PubMed
-
- WHO. WHO Recommendations on Health Promotion Interventions for Maternal and Newborn Health 2015. Geneva: World Health Organization; (2015). Available online at: https://www.who.int/publications/i/item/9789241508742 (Accessed January 1, 2023). - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous