

Evaluating the Reliability of the Lesser Trochanter as a Landmark for Limb Length Discrepancy in Direct Anterior Approach Total Hip Arthroplasty
- PMID: 40772134
- PMCID: PMC12326340
- DOI: 10.7759/cureus.87418
Evaluating the Reliability of the Lesser Trochanter as a Landmark for Limb Length Discrepancy in Direct Anterior Approach Total Hip Arthroplasty
Abstract
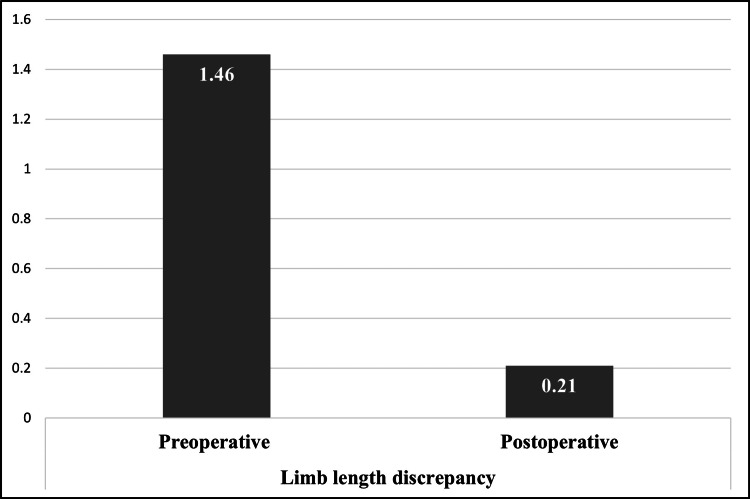
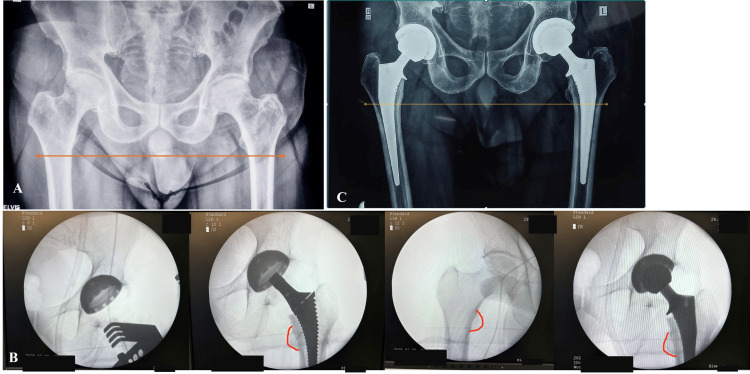
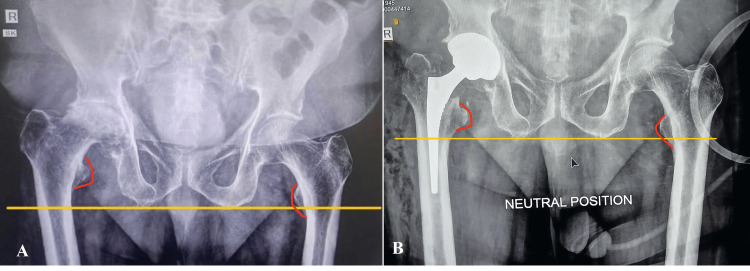
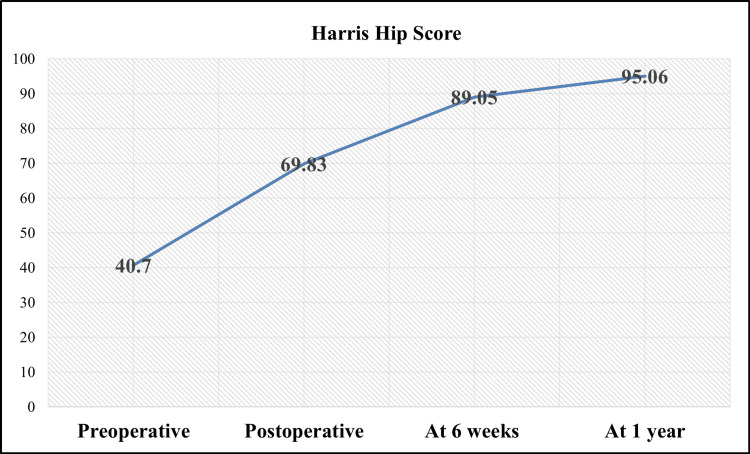
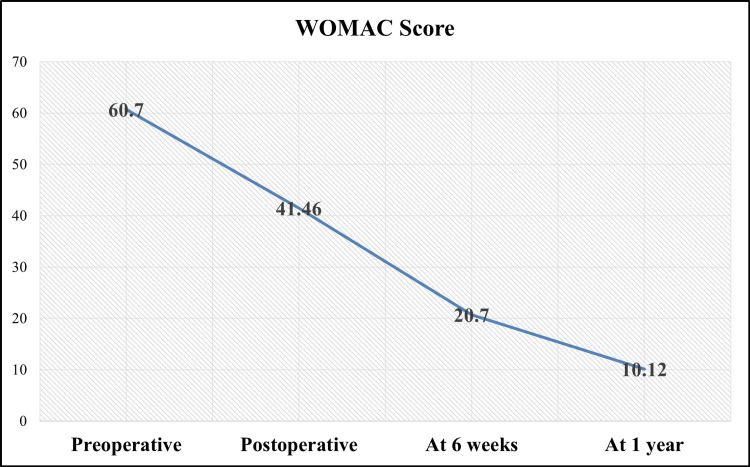
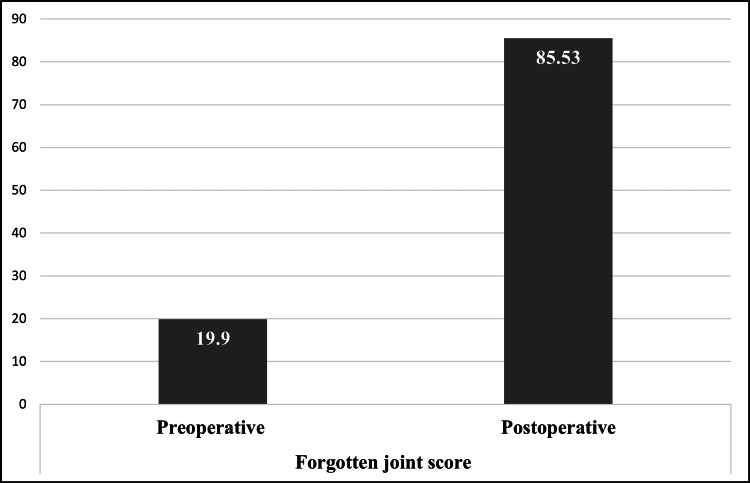
Background and aim Limb length discrepancy (LLD) is a common complication following total hip arthroplasty (THA), significantly impacting functional outcomes, patient satisfaction, and quality of life. The direct anterior approach (DAA) for THA has gained popularity due to its potential for minimizing LLD through precise intraoperative control. Despite advancements, achieving limb length equality remains challenging, particularly in the Indian patient population, where anatomical variations may affect surgical outcomes. The lesser trochanter (LT) is frequently utilized as a landmark for intraoperative LLD assessment. However, the reliability of the LT in DAA-THA remains debated. This study aimed to evaluate the accuracy and consistency of using the LT as an intraoperative reference for LLD correction in DAA-THA. Methods A retrospective cohort analysis was conducted on 130 patients who underwent DAA-THA at a high-volume tertiary care center between January 2023 and December 2023. Patients were selected based on the inclusion criteria of age >18 years, availability of preoperative and postoperative radiographs, and adequate fluoroscopic imaging during surgery. The LT was used as the primary landmark for limb length restoration. Intraoperative fluoroscopy and standardized leg positioning systems were employed to ensure accurate component placement. Preoperative and postoperative LLD were measured using standardized radiographic techniques, and functional outcomes were assessed through the Harris Hip Score (HHS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), and Forgotten Joint Score (FJS). Statistical analysis was performed to determine the association between LLD correction and functional recovery. Results The cohort had a mean age of 57.1 years, with 70% males and 30% females. The mean BMI was 27.1 ± 4.4 kg/m2. Primary indications were avascular necrosis (73.8%), femoral neck fractures (19.2%), rheumatoid arthritis (6.2%), and primary osteoarthritis (0.8%). The mean preoperative LLD of 1.5 cm was reduced to 0.2 cm postoperatively, with only two patients having LLD >1 cm. Functional outcomes improved significantly postoperatively, with HHS increasing from 40.7 ± 5.7 preoperatively to 95.1 ± 4.4 at 12 months (p < 0.001). The WOMAC score decreased from 60.7 ± 5.8 to 10.1 ± 6.7 over the same period (p < 0.001). The FJS improved from 19.9 ± 6.45 preoperatively to 85.5 ± 9.3 postoperatively, indicating high patient satisfaction. Patients with postoperative LLD ≤0.5 cm had significantly higher HHS and lower WOMAC scores compared to those with residual LLD >1 cm, highlighting the importance of precise LLD correction for optimal functional recovery. Conclusion The LT serves as a reliable anatomical landmark for correcting LLD during DAA-THA, particularly when combined with intraoperative fluoroscopy and standardized positioning systems. This approach resulted in favorable postoperative functional outcomes and high patient satisfaction. Implementing standardized protocols that include LT-based measurements and fluoroscopic validation can significantly reduce LLD, enhancing clinical outcomes in THA. Further research is warranted to validate these findings in larger, multicenter cohorts.
Keywords: direct anterior approach; fluoroscopic validation; functional outcomes; lesser trochanter (lt); limb length discrepancy; total hip arthroplasty.
Copyright © 2025, Bajwa et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
What Are the Functional, Radiographic, and Survivorship Outcomes of a Modified Cup-cage Technique for Pelvic Discontinuity?Clin Orthop Relat Res. 2024 Dec 1;482(12):2149-2160. doi: 10.1097/CORR.0000000000003186. Epub 2024 Jul 9. Clin Orthop Relat Res. 2024. PMID: 38991223
-
Surgical Hip Dislocation in the Era of Hip Arthroscopy Demonstrates High Survivorship and Improvements in Patient-reported Outcomes for Complex Femoroacetabular Impingement.Clin Orthop Relat Res. 2024 Sep 1;482(9):1671-1682. doi: 10.1097/CORR.0000000000003032. Epub 2024 Mar 21. Clin Orthop Relat Res. 2024. PMID: 38513108
-
Mini-open Femoroacetabular Osteoplasty in Patients With Tönnis Grade 2 or Higher Osteoarthritis is Associated With a Higher Risk of Subsequent Conversion to THA.Clin Orthop Relat Res. 2024 Sep 1;482(9):1614-1623. doi: 10.1097/CORR.0000000000002944. Epub 2024 Jan 3. Clin Orthop Relat Res. 2024. PMID: 38170724
-
Assistive devices, hip precautions, environmental modifications and training to prevent dislocation and improve function after hip arthroplasty.Cochrane Database Syst Rev. 2016 Jul 4;7(7):CD010815. doi: 10.1002/14651858.CD010815.pub2. Cochrane Database Syst Rev. 2016. PMID: 27374001 Free PMC article.
-
Direct anterior approach versus posterolateral approach for total hip arthroplasty in the treatment of femoral neck fractures in elderly patients: a meta-analysis and systematic review.Ann Med. 2023 Dec;55(1):1378-1392. doi: 10.1080/07853890.2023.2193424. Ann Med. 2023. PMID: 37000019 Free PMC article.
References
-
- Leg length discrepancy after total hip arthroplasty: can leg length be satisfactorily controlled via anterior approach without a traction table? Evaluation in 56 patients with EOS 3D. Lecoanet P, Vargas M, Pallaro J, Thelen T, Ribes C, Fabre T. Orthop Traumatol Surg Res. 2018;104:1143–1148. - PubMed
LinkOut - more resources
Full Text Sources