

Ultrasound vs. Reality: A Multi-centre Study of Real-World Imaging Practices in Suspected Appendicitis in the United Kingdom
- PMID: 40772139
- PMCID: PMC12327546
- DOI: 10.7759/cureus.87445
Ultrasound vs. Reality: A Multi-centre Study of Real-World Imaging Practices in Suspected Appendicitis in the United Kingdom
Abstract
Background: Appendicitis is one of the leading causes for emergency surgery in the United Kingdom (UK), with approximately 50,000 appendectomies performed annually. While imaging plays an increasingly important role in diagnosis, the lack of specific, unified guidelines guiding the utilisation of various imaging modalities causes ambiguity in how and when various modalities should be used.
Objective: This study aimed to evaluate how various imaging modalities are being used in day-to-day practice, the practical aspects, the challenges, and the benefits of one scan over the others. This was done by comparing the diagnostic accuracy of various scans, such as ultrasound (US), CT, and MRI scans in suspected appendicitis cases.
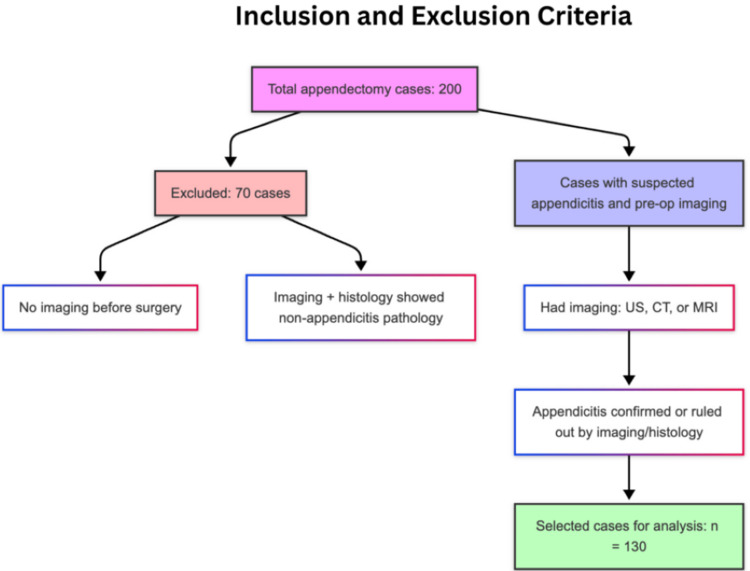
Methods: We retrospectively reviewed 200 recent appendectomy cases across two major hospitals in Manchester. After excluding 70 patients who either had no preoperative imaging or were diagnosed with something other than appendicitis, we analysed the radiology and histopathology reports of the remaining 130 patients. Special attention was given to the subgroup of 52 patients who initially underwent US.
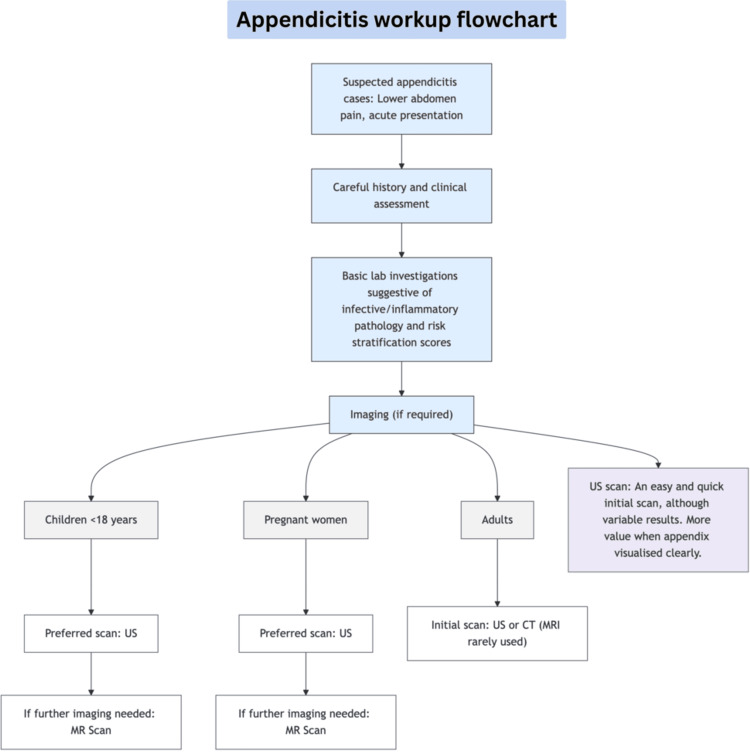
Results: US had a sensitivity (Sn) of 56.25%, with 21 missed diagnoses later confirmed via CT, MRI, or histopathology. US should be commonly used for those under 18, but surprisingly, approximately two-thirds of US cases were adults, representing an inclination to use US as an initial investigation. In the under-18 group, US Sn was 80%, dropping to just 37.5% in the 18-29-year age group. US was not able to visualise the appendix in 34% (n=18) of patients, missing out on many appendicitis diagnoses. The CT scan was the most utilised scan and had a sensitivity of nearly 99%. The MRI scan, although limited in numbers, had a sensitivity of 100%.
Conclusion: While US offers benefits such as speed and no radiation exposure, its diagnostic reliability varies with the patient's body habitus and the operator's skills. The appendix was not identified in a good proportion of patients; however, when the appendix was clearly visualised, it was associated with a better sensitivity. The CT scan was the most utilised scan. It also proved to have excellent sensitivity and is quicker to perform compared to an MRI scan. The MRI scan provides CT equivalent sensitivity but without exposure to harmful radiation. However, it was being underutilised due to limitations in practicality and availability. We routinely request these scans to support the diagnosis of appendicitis, but it is important to understand their diagnostic value, limitations, and when they are most appropriately used.
Keywords: appendectomy; appendicitis; appendicitis diagnostic accuracy; diagnostic approach of appendicitis; imaging in appendicitis cases; imaging of appendix; imaging preference in appendicitis; ultrasound efficacy; ultrasound efficacy in appendicitis.
Copyright © 2025, Vashistha et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Animal subjects: All authors have confirmed that this study did not involve animal subjects or tissue. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Sexual Harassment and Prevention Training.2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Mar 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 36508513 Free Books & Documents.
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
-
Diagnostic test accuracy and cost-effectiveness of tests for codeletion of chromosomal arms 1p and 19q in people with glioma.Cochrane Database Syst Rev. 2022 Mar 2;3(3):CD013387. doi: 10.1002/14651858.CD013387.pub2. Cochrane Database Syst Rev. 2022. PMID: 35233774 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
References
-
- Appendicitis: prevalence. [ Jul; 2025 ];https://cks.nice.org.uk/topics/appendicitis/background-information/preva... 2024 27:2025.
-
- The Royal College of Radiologists. Assessing the diagnostic sensitivity of CT and ultrasound in suspected appendicitis. [ Jul; 2025 ]. 2013. https://www.rcr.ac.uk/career-development/audit-quality-improvement/audit... https://www.rcr.ac.uk/career-development/audit-quality-improvement/audit...
-
- Negative appendectomy rate in the era of CT: an 18-year perspective. Raja AS, Wright C, Sodickson AD, et al. Radiology. 2010;256:460–465. - PubMed
-
- An analysis of time to completion of contrast vs non-contrast computed tomography (CT) scans ordered in a large public emergency department. Lee MB, Pyle M. https://www.annemergmed.com/article/S0196-0644(24)00774-1/fulltext Ann Emerg Med. 2024;84:0.
-
- The Royal College of Radiologists. 2023 clinical radiology and clinical oncology workforce census reports. [ Jul; 2025 ]. 2024. https://www.rcr.ac.uk/news-policy/latest-updates/2023-clinical-radiology... https://www.rcr.ac.uk/news-policy/latest-updates/2023-clinical-radiology...
LinkOut - more resources
Full Text Sources