

Minimally Invasive Approach to Intrauterine Device Migration Into the Bladder Using Holmium Laser
- PMID: 40772142
- PMCID: PMC12325757
- DOI: 10.7759/cureus.87377
Minimally Invasive Approach to Intrauterine Device Migration Into the Bladder Using Holmium Laser
Abstract
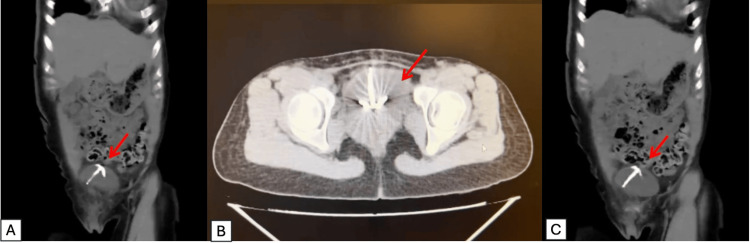
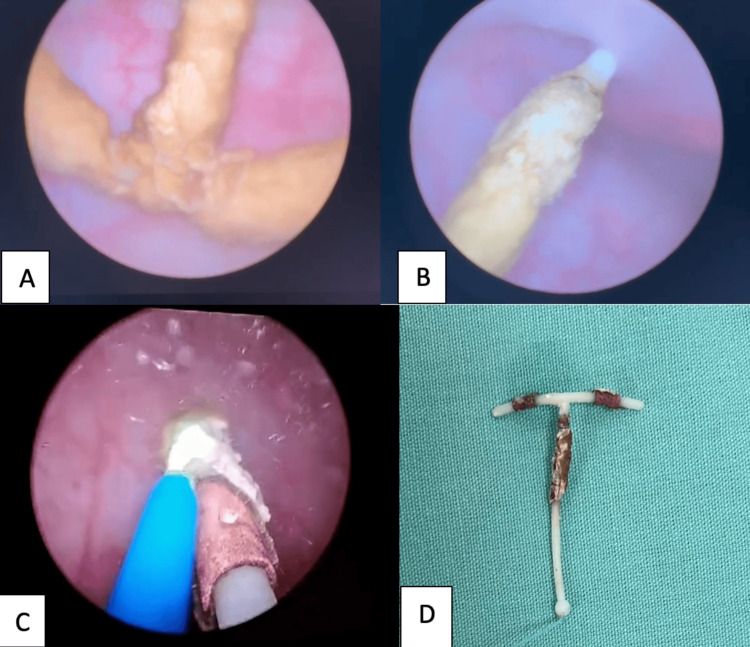
The intrauterine device (IUD) is a widely utilized method of contraception known for its high efficacy, safety profile, and long-term effectiveness. Despite its favorable characteristics, rare but potentially serious complications may occur, such as uterine perforation and device migration into adjacent pelvic or abdominal structures. One of the less frequent but clinically relevant complications is intravesical migration, where the device perforates the uterine wall and erodes into the urinary bladder. This can result in chronic lower urinary tract symptoms, recurrent urinary tract infections, hematuria, pelvic discomfort, and, in some cases, stone formation around the foreign body. We present the case of a 26-year-old female patient who developed recurrent urinary symptoms and intermittent hematuria three years after IUD placement. The device had not been visualized during gynecological follow-up and remained undetected during two full-term pregnancies. A noncontrast abdominal CT scan ultimately revealed a calcified IUD located within the urinary bladder. The patient underwent successful transurethral endoscopic removal using holmium:YAG laser lithotripsy in dusting mode to fragment the calcifications, followed by retrieval of the intact device with foreign body forceps. The procedure was completed without complications, and the patient reported full resolution of symptoms during follow-up. This case underscores the importance of considering IUD migration as a differential diagnosis in women presenting with unexplained urinary symptoms and a remote history of IUD use. It also demonstrates that holmium laser-assisted endoscopic management provides a safe, effective, and minimally invasive approach to remove encrusted or calcified intravesical IUDs, avoiding the need for open or laparoscopic surgery.
Keywords: copper intrauterine device; endoscopic removal; holmium:yag laser; intravesical foreign body; migrated intrauterine device; minimally invasive surgery; recurrent urinary tract infection; urinary bladder.
Copyright © 2025, Torres Zapata et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Not applicable-single case report with informed consent obtained issued approval Not applicable. This case report did not require IRB or ethics committee approval as it describes a single clinical case. Informed consent was obtained from the patient for publication. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Management of urinary stones by experts in stone disease (ESD 2025).Arch Ital Urol Androl. 2025 Jun 30;97(2):14085. doi: 10.4081/aiua.2025.14085. Epub 2025 Jun 30. Arch Ital Urol Androl. 2025. PMID: 40583613 Review.
-
Invasive urodynamic investigations in the management of women with refractory overactive bladder symptoms: FUTURE, a superiority RCT and economic evaluation.Health Technol Assess. 2025 Jul;29(27):1-139. doi: 10.3310/UKYW4923. Health Technol Assess. 2025. PMID: 40620147 Free PMC article. Clinical Trial.
-
Immediate postabortal insertion of intrauterine devices.Cochrane Database Syst Rev. 2002;(3):CD001777. doi: 10.1002/14651858.CD001777. Cochrane Database Syst Rev. 2002. Update in: Cochrane Database Syst Rev. 2004 Oct 18;(4):CD001777. doi: 10.1002/14651858.CD001777.pub2. PMID: 12137634 Updated.
-
Case Report: Strangulated intestinal obstruction due to chronic migration of an intrauterine device (IUD): a 30-year latent complication.Front Med (Lausanne). 2025 Jul 7;12:1613116. doi: 10.3389/fmed.2025.1613116. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40692957 Free PMC article.
-
Traditional suburethral sling operations for urinary incontinence in women.Cochrane Database Syst Rev. 2017 Jul 26;7(7):CD001754. doi: 10.1002/14651858.CD001754.pub4. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 28;1:CD001754. doi: 10.1002/14651858.CD001754.pub5. PMID: 28743177 Free PMC article. Updated.
References
-
- Uterine perforation caused by intrauterine devices: clinical course and treatment. Kaislasuo J, Suhonen S, Gissler M, Lähteenmäki P, Heikinheimo O. Hum Reprod. 2013;28:1546–1551. - PubMed
-
- Complete and partial uterine perforation and embedding following insertion of intrauterine devices. I. Classification, complications, mechanism, incidence, and missing string. Zakin D, Stern WZ, Rosenblatt R. https://journals.lww.com/obgynsurvey/citation/1981/08000/Complete_and_Pa.... Obstet Gynecol Surv. 1981;36:335–353. - PubMed
-
- Extrauterine mislocated IUD: is surgical removal mandatory? Markovitch O, Klein Z, Gidoni Y, Herman A, Pansky M. Contraception. 2002;65:105–108. - PubMed
-
- Family planning/contraception methods. 2025. https://www.who.int/news-room/fact-sheets/detail/family-planning-contrac... https://www.who.int/news-room/fact-sheets/detail/family-planning-contrac...
Publication types
LinkOut - more resources
Full Text Sources