

Situs Inversus Totalis: Challenges and Anatomical Considerations in Endoscopic Retrograde Cholangiopancreatography
- PMID: 40772152
- PMCID: PMC12327922
- DOI: 10.7759/cureus.87427
Situs Inversus Totalis: Challenges and Anatomical Considerations in Endoscopic Retrograde Cholangiopancreatography
Abstract
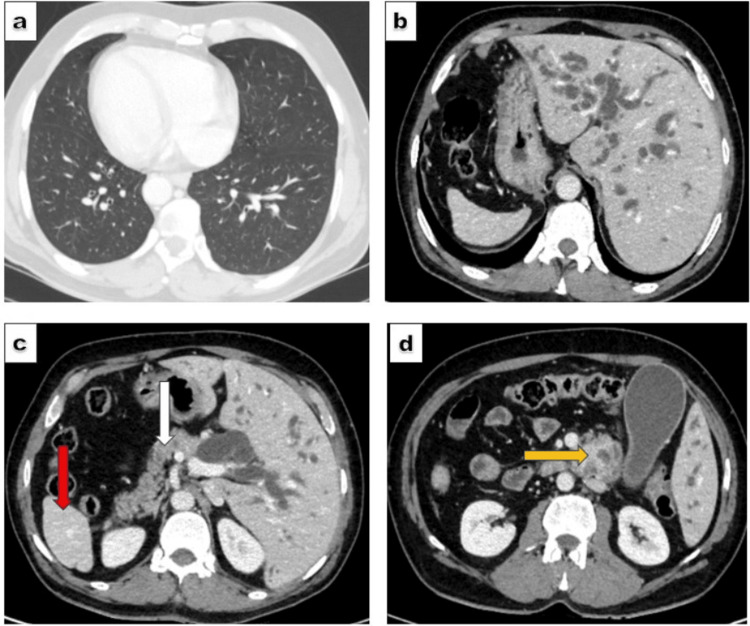
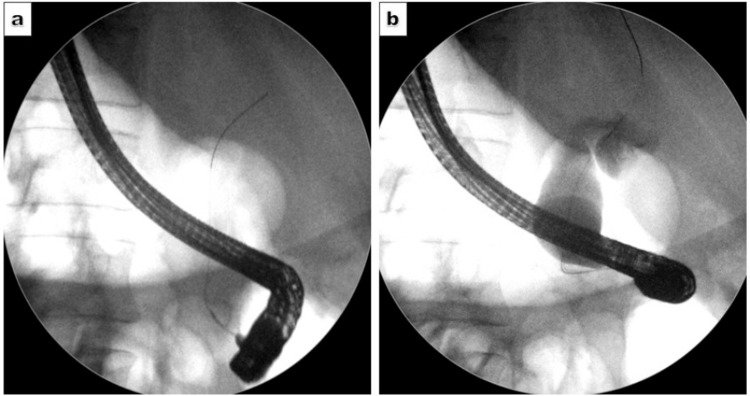
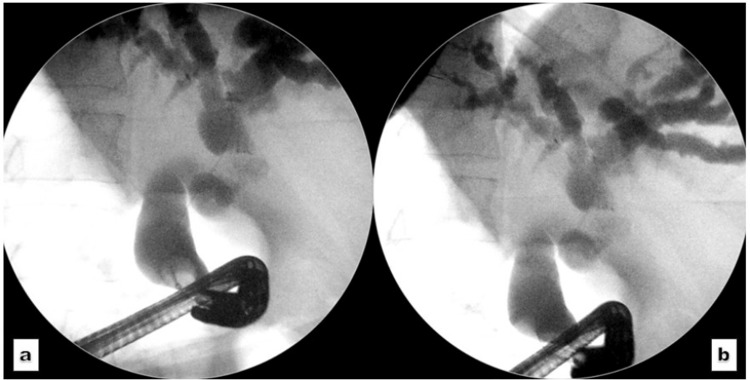
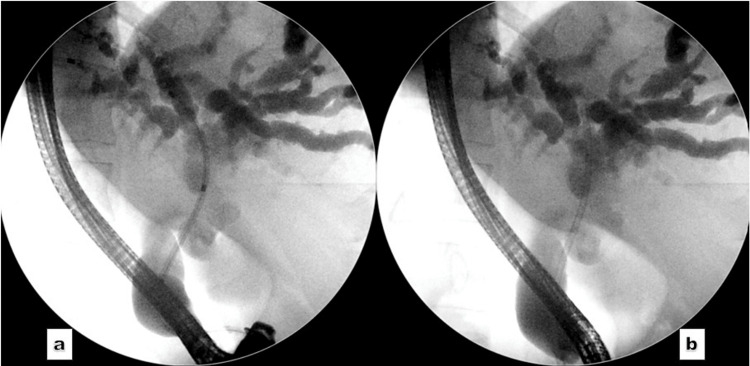
Situs inversus totalis (SIT) is a rare condition characterised by the reversed positioning of abdominal and thoracic viscera. The anomaly poses a significant anatomical challenge during routine endoscopic procedures, including endoscopic retrograde cholangiopancreatography (ERCP). Here, we present the case of a 51-year-old patient with SIT and obstructive jaundice due to a periampullary mass. Initial ERCP attempts at an external facility for biliary decompression were unsuccessful, prompting referral to our center. Multidisciplinary consensus recommended preoperative ERCP followed by a Whipple's procedure. ERCP was performed with positional adjustments (prone position) of the patient and significant scope manipulation (stepwise 360-degree anticlockwise rotation) to navigate the reversed anatomy. Cannulation was achieved, and a plastic biliary stent was placed, resulting in effective drainage. The patient demonstrated clinical improvement and was referred for surgical intervention. A comprehensive understanding of the reversed anatomy, along with the operator's skill and experience, is essential to address the challenges posed by this unique anatomical variation.
Keywords: cholangiocarcinoma; common bile duct; endoscopic retrograde cholangiopancreatography; reversed anatomy; situs inversus totalis.
Copyright © 2025, Aujla et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Pakistan Kidney and Liver Institute and Research Center, Institutional Review Board issued approval PKLI-IRB/AP/00032025. The case was submitted to the IRB. Exemption was granted to publish the paper. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Laparoscopic Cholecystectomy in Situs Inversus Totalis With Combined Indocyanine Green Fluorescence and Conventional Cholangiography: A Case Report.Cureus. 2025 Jun 25;17(6):e86761. doi: 10.7759/cureus.86761. eCollection 2025 Jun. Cureus. 2025. PMID: 40718221 Free PMC article.
-
NIH state-of-the-science statement on endoscopic retrograde cholangiopancreatography (ERCP) for diagnosis and therapy.NIH Consens State Sci Statements. 2002 Jan 14-16;19(1):1-26. NIH Consens State Sci Statements. 2002. PMID: 14768653
-
Endoscopic retrograde cholangiopancreatography for the treatment of common bile duct dilatation with choledocholithiasis in children: a single-center retrospective cohort study of 58 cases.BMC Pediatr. 2025 Jul 5;25(1):535. doi: 10.1186/s12887-025-05888-y. BMC Pediatr. 2025. PMID: 40618040 Free PMC article.
-
Endoscopic retrograde cholangiopancreatography treatment of cholangitis stone in a patient with total situs inversus: A case report.World J Gastrointest Endosc. 2025 Jun 16;17(6):106347. doi: 10.4253/wjge.v17.i6.106347. World J Gastrointest Endosc. 2025. PMID: 40547559 Free PMC article.
-
Endoscopic retrograde cholangiopancreatography versus intraoperative cholangiography for diagnosis of common bile duct stones.Cochrane Database Syst Rev. 2015 Feb 26;2015(2):CD010339. doi: 10.1002/14651858.CD010339.pub2. Cochrane Database Syst Rev. 2015. PMID: 25719222 Free PMC article.
References
-
- When cilia go bad: cilia defects and ciliopathies. Fliegauf M, Benzing T, Omran H. Nat Rev Mol Cell Biol. 2007;8:880–893. - PubMed
-
- Congenital heart disease and other heterotaxic defects in a large cohort of patients with primary ciliary dyskinesia. Kennedy MP, Omran H, Leigh MW, et al. Circulation. 2007;115:2814–2821. - PubMed
Publication types
LinkOut - more resources
Full Text Sources