

John Cunningham (JC) Virus Encephalitis Without Progressive Multifocal Leukoencephalopathy in a Stem Cell Transplant Patient: A Case Report and Literature Review
- PMID: 40772164
- PMCID: PMC12327955
- DOI: 10.7759/cureus.87464
John Cunningham (JC) Virus Encephalitis Without Progressive Multifocal Leukoencephalopathy in a Stem Cell Transplant Patient: A Case Report and Literature Review
Abstract
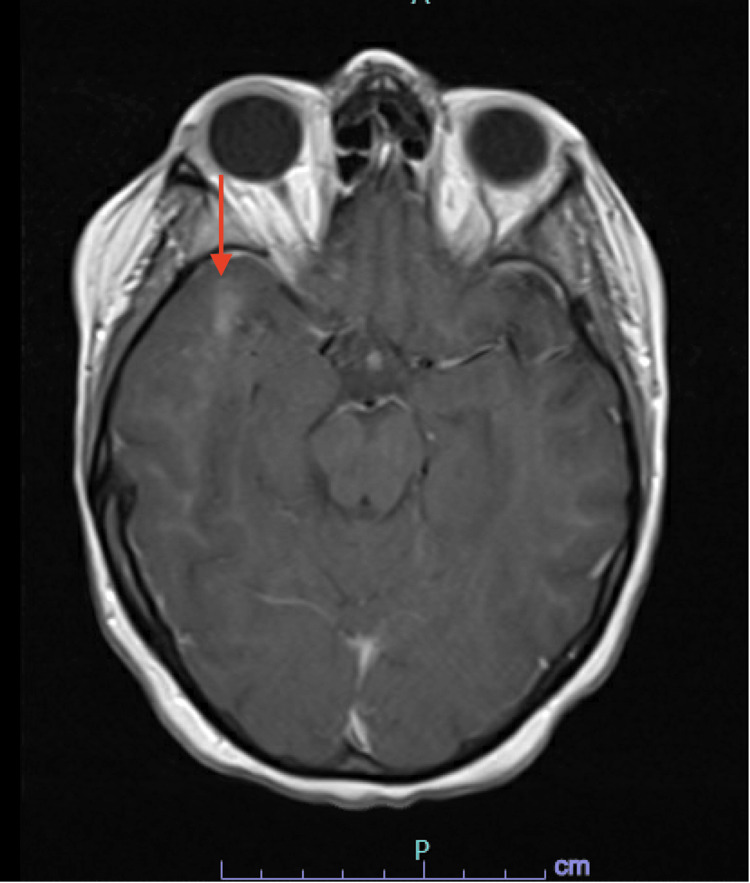
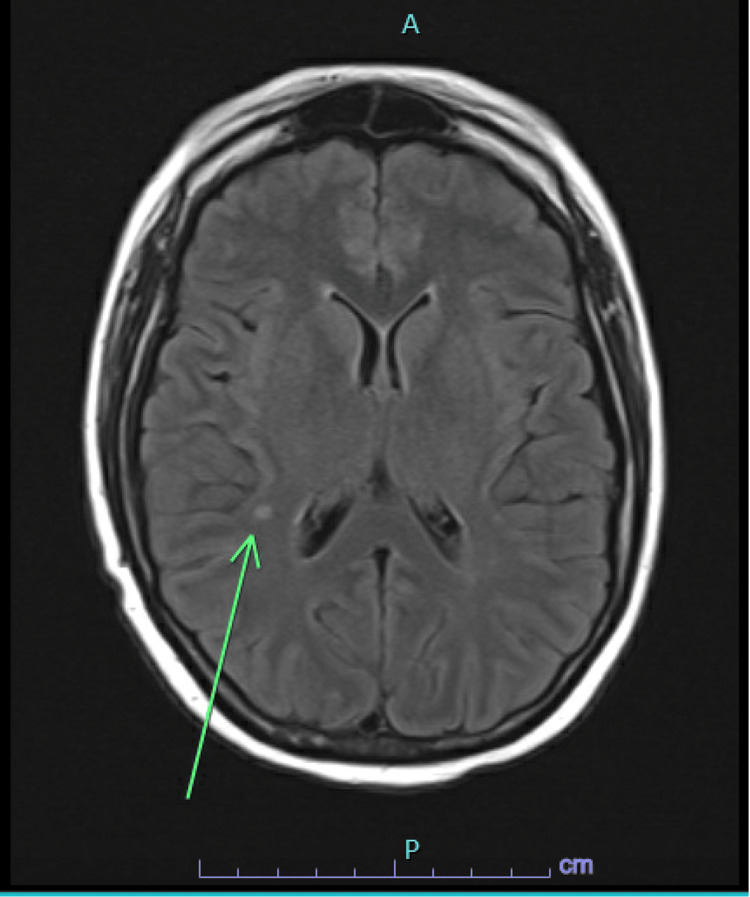
John Cunningham (JC) Virus (JCV) belongs to the Polyomaviridae family and is notorious for remaining latent in the kidneys and lymphoid organs of healthy populations. However, in the setting of profound immunosuppression, the virus can reactivate, leading to various manifestations depending on its location of infection, i.e., progressive multifocal leukoencephalopathy (PML), JC virus encephalopathy, or JC virus granule cell neuronopathy. Here, we present a unique case of a 28-year-old female with a notable medical history of acute myeloid leukemia (AML) status post stem cell transplant who presented to the emergency department (ED) for evaluation of her altered mental status for one week. Laboratory investigations documented the presence of JCV in both the blood and cerebrospinal fluid (CSF). Unlike the typical findings of PML, the brain imaging revealed a 4 mm T2-weighted fluid attenuated inversion recovery (T2/FLAIR) hyperintense enhancing focus in the right supratentorial region and a right anterior temporal subcortical white matter enhancement measuring up to 14 mm in size with no corresponding FLAIR abnormality suggestive of JCV encephalitis. The patient received virus-specific T cells but showed minimal to no improvement. Hence, the patient's family opted for hospice care, but the patient died subsequently. JCV encephalitis is a relatively rare condition; only a few case reports have been reported. The prognosis of JCV encephalitis is not well established and is most often lethal with high viral loads. Virus-specific T-cell therapy has not yet demonstrated the desired clinical benefit; therefore, additional data are required.
Keywords: acute myeloid leukemia; encephalitis; jc virus; progressive multifocal leukoencephalopathy; stem cell.
Copyright © 2025, Fatima et al.
Conflict of interest statement
Human subjects: Informed consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Cultivation of papova-like virus from human brain with progressive multifocal leucoencephalopathy. Padgett B, Zurhein G, Walker D, Eckroade R, Dessel B. Lancet. 1971;297:1257–1260. - PubMed
-
- Progressive multifocal leukoencephalopathy: why gray and white matter. Gheuens S, Wüthrich C, Koralnik IJ. Annu Rev Pathol. 2013;8:189–215. - PubMed
-
- Progressive multifocal leukoencephalopathy deaths in the USA, 1979-2005. Christensen KL, Holman RC, Hammett TA, Belay ED, Schonberger LB. Neuroepidemiology. 2010;35:178–184. - PubMed
Publication types
LinkOut - more resources
Full Text Sources