

Impact of bile duct stenting on the management of symptomatic choledocholithiasis: a retrospective multicenter analysis
- PMID: 40772258
- PMCID: PMC12325275
- DOI: 10.3389/fsurg.2025.1630416
Impact of bile duct stenting on the management of symptomatic choledocholithiasis: a retrospective multicenter analysis
Abstract
Objective: Choledocholithiasis (CDL) can lead to various complications and requires treatment approaches for both biliary tract clearing and cholecystectomy. This study aims to characterize CDL patients, evaluate treatment strategies, assess associated complications, and explore economic impacts.
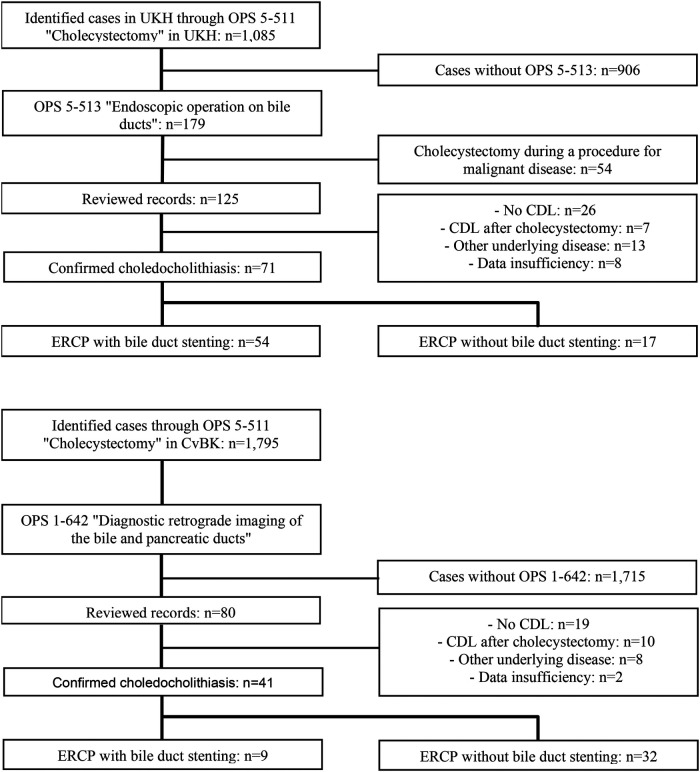
Methods: We conducted a retrospective analysis of 112 patients between 2016 and 2021 at two centers. We performed a descriptive analysis comparing outcomes of patients undergoing ERCP with and without bile duct stenting. Univariate and multivariable analyses were used to identify factors related to complications.
Results: Bile duct stenting was associated with significantly higher complication rates (52.4%) compared to the group without stenting (26.5%) (p = 0.006). Factors influencing stent implantation included prior abdominal surgeries (OR = 03.51, p = 0.02), cholangitis at admission (OR = 03.02, p = 0.032), and bile duct diameter (OR = 01.16, p = 0.057). The overall median length of stay was longer for patients with stenting (19 days) compared to those without (11 days) (p < 0.001). Finally, reimbursements were higher for patients with stenting. Reimbursement for complicated courses was higher than for those without, independent of initial bile duct stenting (with stent p = 0.006, without stent p = 0,003).
Conclusion: Bile duct stenting during CDL management is associated with higher complication rates, longer hospital stay, and increased costs. These associations may reflect both clinical severity at baseline and procedural sequencing. A more restrictive placement of biliary stents might be advisable.
Keywords: ERCP; cholecysititis; cholecystectomy; stent; surgery.
© 2025 Rebelo, Tischer, Rosendahl, Walldorf, Mosa, Kleeff and Klose.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Endoscopic retrograde cholangiopancreatography versus intraoperative cholangiography for diagnosis of common bile duct stones.Cochrane Database Syst Rev. 2015 Feb 26;2015(2):CD010339. doi: 10.1002/14651858.CD010339.pub2. Cochrane Database Syst Rev. 2015. PMID: 25719222 Free PMC article.
-
Surgical versus endoscopic treatment of bile duct stones.Cochrane Database Syst Rev. 2013 Dec 12;2013(12):CD003327. doi: 10.1002/14651858.CD003327.pub4. Cochrane Database Syst Rev. 2013. PMID: 24338858 Free PMC article.
-
Surgical versus endoscopic treatment of bile duct stones.Cochrane Database Syst Rev. 2013 Sep 3;(9):CD003327. doi: 10.1002/14651858.CD003327.pub3. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2013 Dec 12;(12):CD003327. doi: 10.1002/14651858.CD003327.pub4. PMID: 23999986 Updated.
-
Primary closure versus T-tube drainage after open common bile duct exploration.Cochrane Database Syst Rev. 2007 Jan 24;(1):CD005640. doi: 10.1002/14651858.CD005640.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2013 Jun 21;(6):CD005640. doi: 10.1002/14651858.CD005640.pub3. PMID: 17253565 Updated.
-
Ultrasound versus liver function tests for diagnosis of common bile duct stones.Cochrane Database Syst Rev. 2015 Feb 26;2015(2):CD011548. doi: 10.1002/14651858.CD011548. Cochrane Database Syst Rev. 2015. PMID: 25719223 Free PMC article.
References
-
- National Institute for Health and Care Excellence (NICE), Gallstone Disease: Diagnosis and Management of Cholelithiasis, Cholecystitis and Choledocholithiasis. (2014). Available online at: https://www.nice.org.uk/guidance/cg188 (Accessed 20 October 2024) - PubMed
-
- Gutt C, Jenssen C, Barreiros AP, Götze TO, Stokes CS, Jansen PL, et al. Updated S3-guideline for prophylaxis, diagnosis and treatment of gallstones. German society for digestive and metabolic diseases (DGVS) and German society for surgery of the alimentary tract (DGAV)—AWMF registry 021/008. Z Gastroenterol. (2018) 56:912–66. 10.1055/a-0644-2972 - DOI - PubMed
LinkOut - more resources
Full Text Sources