

Flap size as a confounding variable in flap perfusion measurement with the Oxygen-to-see (O2C) analysis system in microvascular head and neck reconstruction - a retrospective analysis
- PMID: 40773108
- PMCID: PMC12331801
- DOI: 10.1007/s00784-025-06468-1
Flap size as a confounding variable in flap perfusion measurement with the Oxygen-to-see (O2C) analysis system in microvascular head and neck reconstruction - a retrospective analysis
Abstract
Objectives: The Oxygen-to-see (O2C) analysis system is used for flap monitoring based on predefined threshold values for flap perfusion. However, flap size may be a confounding variable. The aim of this study was to investigate the relationship between flap size and flap perfusion in microvascular head and neck reconstruction.
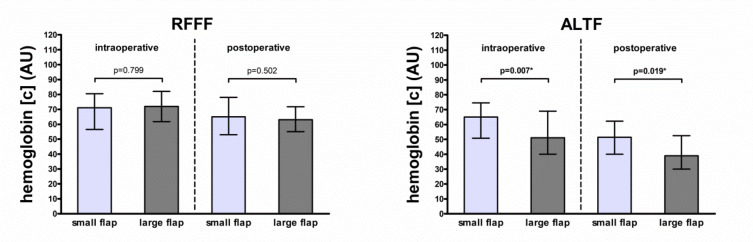
Materials and methods: Flap perfusion values measured with the O2C analysis system between 2011 and 2020 in 252 patients undergoing microvascular head and neck reconstruction with a radial free forearm flap (RFFF) or anterolateral thigh flap (ALTF) were retrospectively analyzed. Intraoperative and postoperative flap blood flow, hemoglobin concentration, and hemoglobin oxygen saturation at 8- and 2-mm tissue depths were compared between small (≤ median flap size) and large flaps (> median flap size) for RFFFs and ALTFs separately.
Results: Intraoperative and postoperative hemoglobin concentration at a 2-mm tissue depth differed between small and large ALTFs (65.0 arbitrary units [AU] vs. 51.0 AU, p = 0.007; and 51.5 AU vs. 39.0 AU, p = 0.019). Both differences persisted in multivariable analysis (p < 0.001 and p = 0.012). Other differences were not observed or did not persist in multivariable analysis for RFFFs and ALTFs (all p > 0.05).
Conclusions: Microvascular free flap perfusion is not related to flap size in terms of flap blood flow and hemoglobin oxygen saturation. This underscores the validity of predefined absolute threshold values in the context of flap monitoring based on perfusion measurement with the O2C analysis system.
Clinical relevance: Flap perfusion measurement with the Oxygen-to-see (O2C) analysis system can be used for flap monitoring of small and large flaps.
Keywords: Flap perfusion monitoring; Flap size; Free flap; Microvascular head and neck reconstruction; Oxygen-to-see analysis system.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: This retrospective chart review study involving human participants was in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the local ethics committee of the Medical Faculty RWTH Aachen University (EK 309 − 20). Competing interests: The authors declare no competing interests. Conflict of interests: The authors declare that they have no conflict of interest regarding the results published in this article.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
