

Improving pediatric care in Uganda with a digital platform and quality improvement initiative: A retrospective review of Smart Triage + QI
- PMID: 40773450
- PMCID: PMC12331088
- DOI: 10.1371/journal.pone.0329369
Improving pediatric care in Uganda with a digital platform and quality improvement initiative: A retrospective review of Smart Triage + QI
Abstract
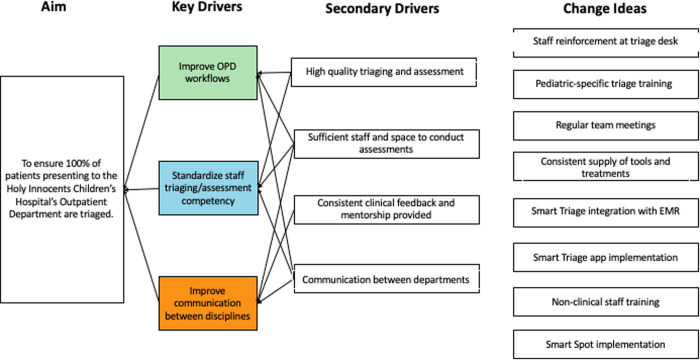
Objective: This is a retrospective review of the feasibility study and implementation of the Smart Triage and Quality Improvement (QI) initiative at Holy Innocents Children's Hospital (HICH), a dedicated pediatric hospital in Mbarara, Uganda, over a 5-year period. The aim of this QI initiative was to improve triaging rates and the time-to-antimicrobials in HICH's outpatient department (OPD).
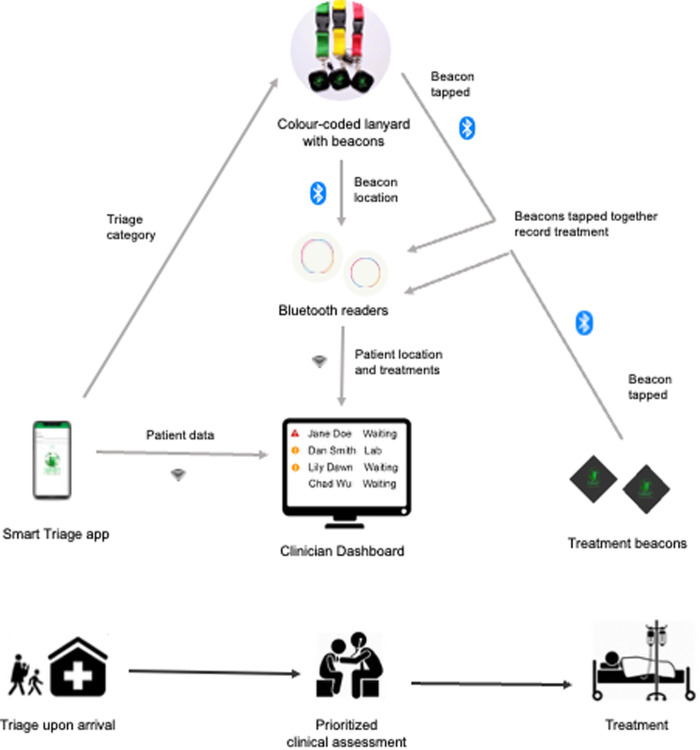
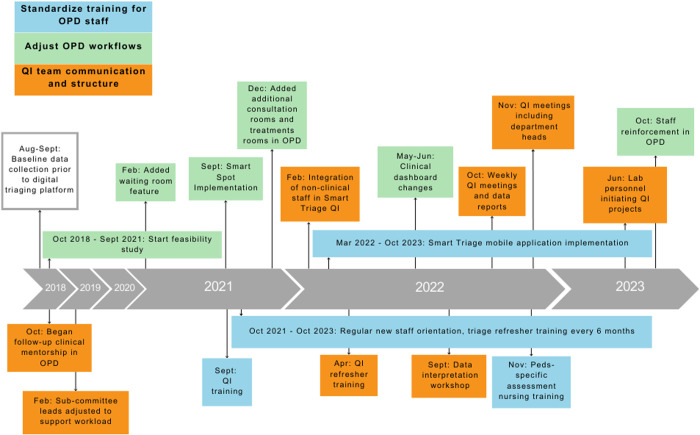
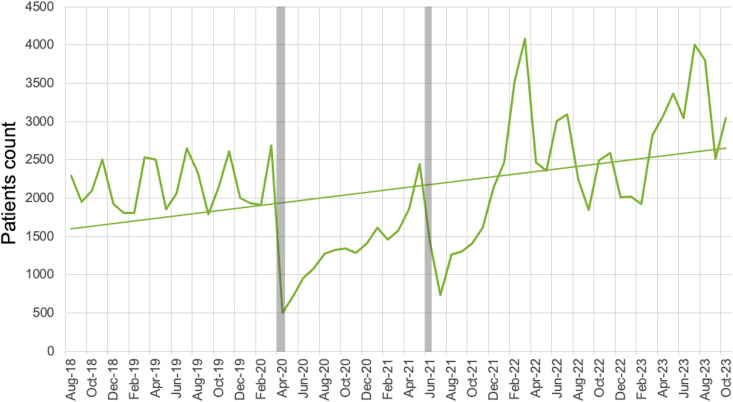
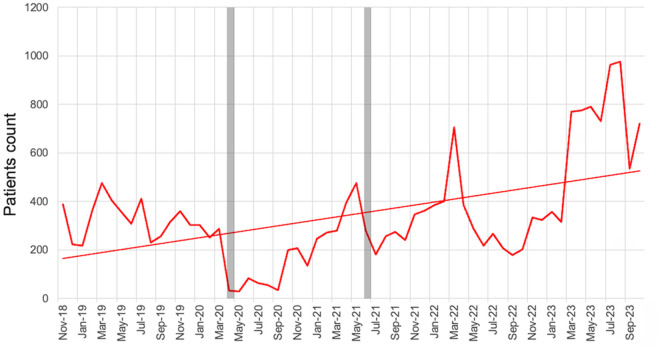
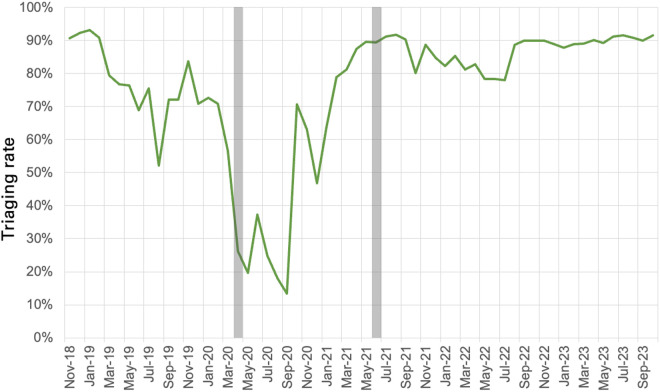
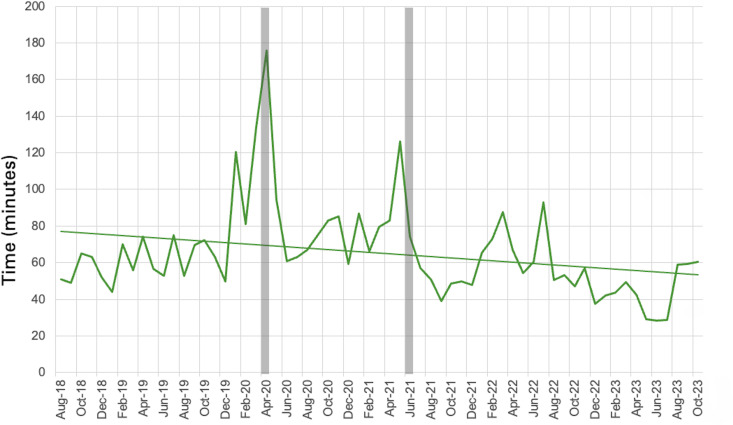
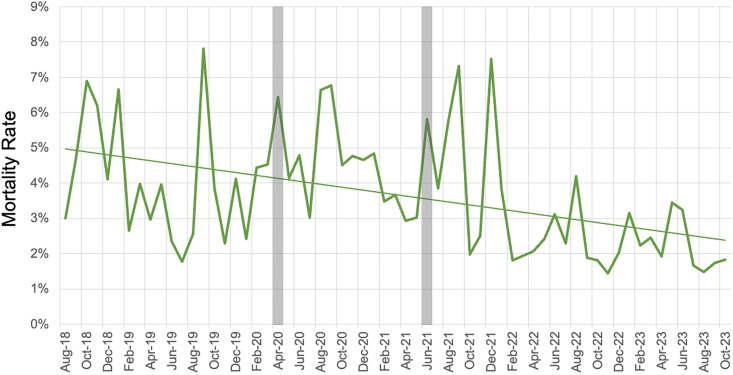
Methods: Smart Triage is a risk prediction algorithm and digital platform that enables healthcare workers to triage patients and track treatments effectively. Following the feasibility study, the QI program was implemented in September 2021 using three Plan-Do-Study-Act cycles: 1) Standardize Training, 2) Adjust Workflows, and 3) QI Team Communication. Data sources were triage and hospital reports. Monthly run charts of OPD attendance, acuity of illness, triaging rates, median-time-to-antimicrobials, and mortality rates of admitted patients were created. The trajectories of the variables were assessed using linear regression with time as the explanatory variable.
Results: 121,521 children attended HICH OPD from November 2018 to October 2023. The OPD triaging rate increased to 91% by October 2023, with a sustained plateau above 90% since July 2022. There was a significant reduction in the median time-to-antimicrobials during the 5-year period, from 77.6 to 53.6 minutes, with a slope of -0.4 minutes per month (CI: -0.73 to -0.04, p-value: 0.029). The inpatient mortality rate decreased from 5.1% in August 2018 to 2.6% in October 2023, with a significant increase in the number of cases with comparable illness severity.
Conclusion: The impact of Smart Triage was sustained beyond the end of the feasibility trial and showed sustained improvements in processes such as treatment times and clinical outcomes including a reduction in mortality. HICH's leadership integrated a culture of QI across disciplines and departments, contributing to this initiative's sustainability and impact.
Copyright: © 2025 Goertzen et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Weiss SL, Peters MJ, Alhazzani W, Agus MSD, Flori HR, Inwald DP, et al. Surviving sepsis campaign international guidelines for the management of septic shock and Sepsis-Associated organ dysfunction in children. Pediatr Crit Care Med. 2020;21(2). - PubMed
-
- Chiotos K, Weiss SL. A wrinkle in time to antibiotics in sepsis: when should one hour be the goal? J Pediatr. 2021;233:13–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
