

Geographical shifting of cholera burden in Africa and its implications for disease control
- PMID: 40775053
- PMCID: PMC12532610
- DOI: 10.1038/s41591-025-03847-9
Geographical shifting of cholera burden in Africa and its implications for disease control
Abstract
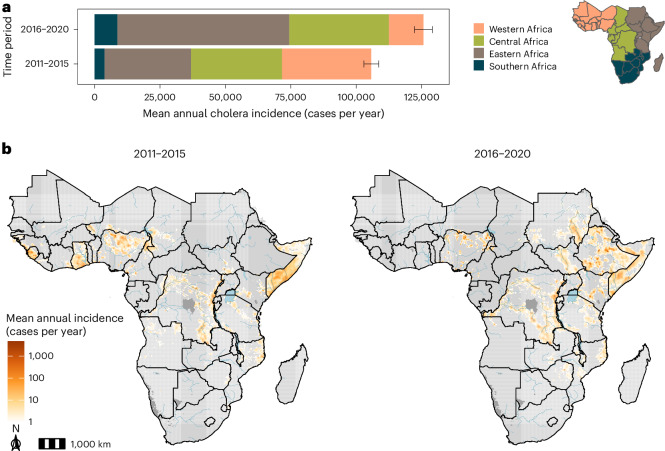
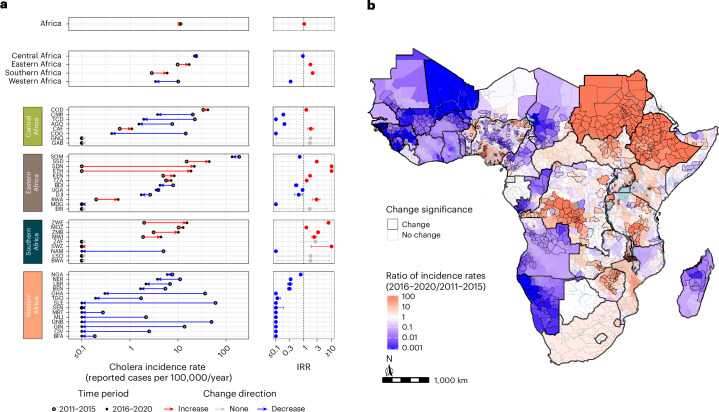
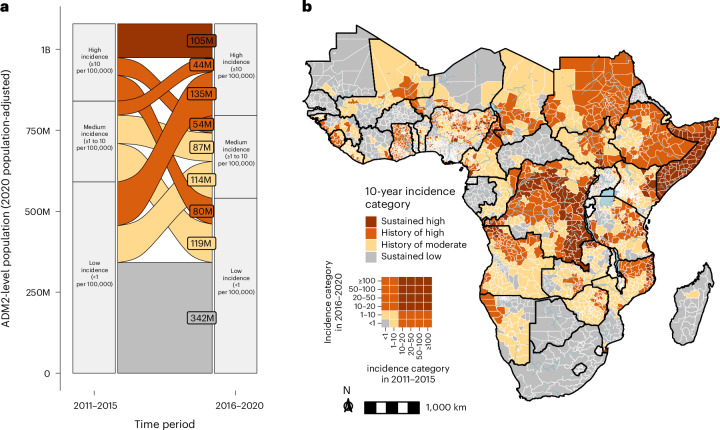
Cholera outbreaks cause substantial morbidity and mortality in Africa, yet changes in the geographic distribution of cholera burden over time remain uncharacterized. We used surveillance data and spatial statistical models to estimate the mean annual incidence of reported suspected cholera for 2011-2015 and 2016-2020 on a 20-km grid across Africa. Across 43 countries, mean annual incidence rates remained at 11 cases per 100,000 population, with 125,701 cases estimated annually (95% credible interval (CrI): 124,737-126,717) from 2016 to 2020. Cholera incidence shifted from western to eastern Africa. There were 296 million people (95% CrI: 282-312 million) in high-incidence second-level administrative (ADM2) units (≥10 cases per 100,000 per year) in 2020, 135 million of whom experienced low incidence (<1 per 100,000) in 2011-2015. ADM2 units with high incidence in central and eastern Africa from 2011 to 2020 were more likely to report cholera in 2022-2023. In hypothetical scenarios of preventive disease control planning, targeting the 100 million highest-burden populations had potential to reach up to 63% of 2016-2020 mean annual cases but only 37% when targeting by past incidence. This retrospective analysis highlights spatiotemporal instability in cholera burden and can be used as a benchmark for tracking future progress in disease control.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: Several authors participate regularly in meetings or are members of the Global Task Force on Cholera Control Surveillance and Oral Cholera Vaccine Working Groups, which provide technical expertise on cholera surveillance and oral cholera vaccine use. A.S.A. is a member of the Gavi Independent Review Committee.
Figures












References
-
- Multi-Country Outbreak of Cholera, External Situation Report #1 - 28 March 2023 (World Health Organization, 2023); https://www.who.int/publications/m/item/multi-country-outbreak-of-choler...
-
- Multi-Country Outbreak of Cholera, External Situation Report #13 - 17 April 2024 (World Health Organization, 2024); https://www.who.int/publications/m/item/multi-country-outbreak-of-choler...
-
- Shortage of cholera vaccines leads to temporary suspension of two-dose strategy, as cases rise worldwide. World Health Organizationhttps://www.who.int/news/item/19-10-2022-shortage-of-cholera-vaccines-le... (2022).
-
- World Health Organization. Cholera, 2022. Wkly Epidemiol. Rec.98, 431–443 (2023).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
