

Efficacy and safety of midazolam compared to fentanyl as adjuvants to hyperbaric bupivacaine in spinal anesthesia: a systematic review and meta-analysis of randomized controlled trials
- PMID: 40775683
- PMCID: PMC12330165
- DOI: 10.1186/s12871-025-03261-1
Efficacy and safety of midazolam compared to fentanyl as adjuvants to hyperbaric bupivacaine in spinal anesthesia: a systematic review and meta-analysis of randomized controlled trials
Abstract
Background: Various drugs have been used as adjuvants to local anesthetics to prolong analgesia and reduce the dosage and side effects of local anesthetics in regional anesthesia and peripheral nerve blocks.
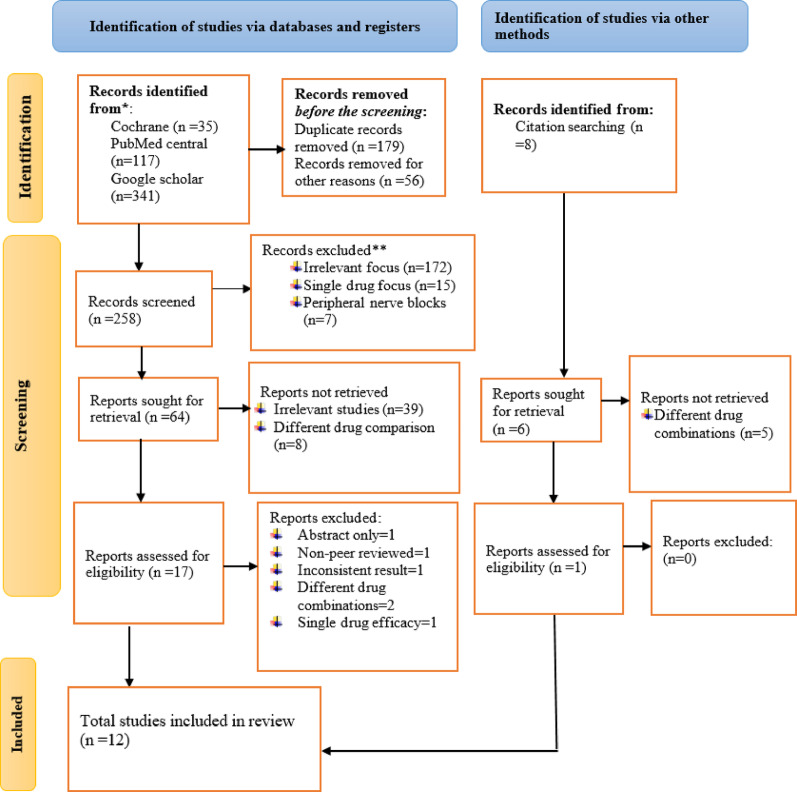
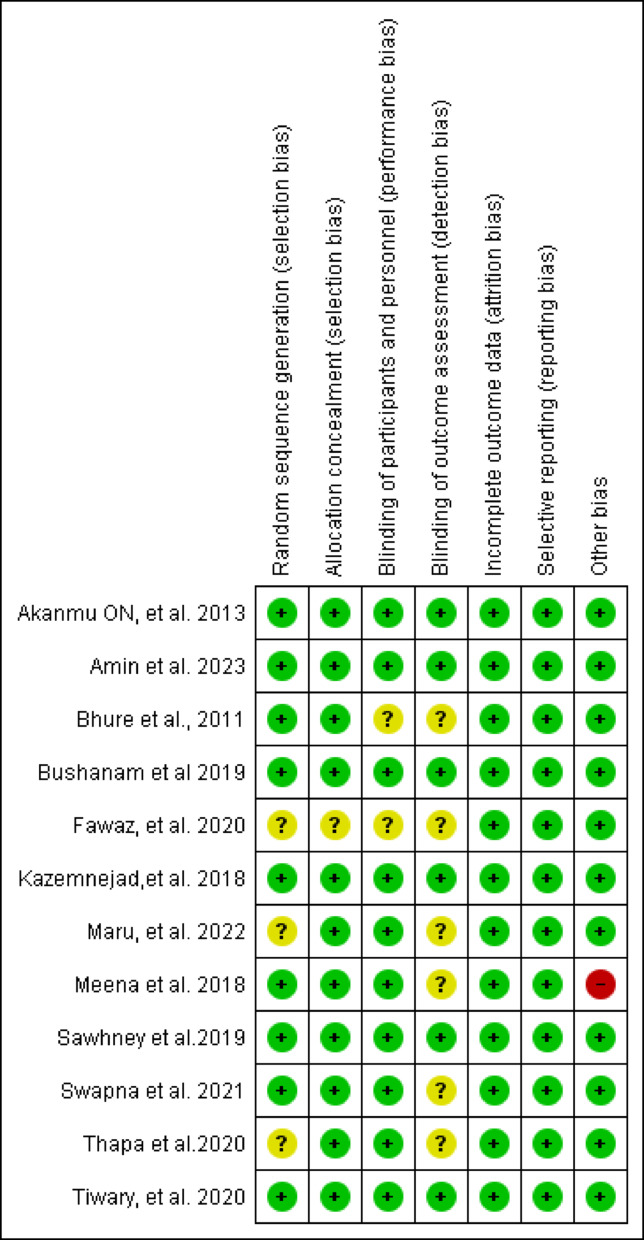
Methods: The literature search was conducted using Google Scholar, PubMed, and the Cochrane Library for randomized controlled trials comparing fentanyl or midazolam to bupivacaine in spinal anesthesia. Studies that reported any of the primary outcomes, duration of sensory block, analgesia and motor block were included. Safety parameters and postoperative pain were the secondary outcomes. The risk of bias and publication bias were assessed using the Cochrane risk of bias tool and Egger's test respectively. A p-value less than 0.05 at 95% confidence interval indicated statistical significance.
Results: This meta-analysis included 12 RCT studies (n = 812). Seven studies (n = 498) reported duration of sensory block and found no significant difference between the groups (MD = 12.18 min; 95% CI- 9.97, 34.34; I2 = 99%). Eleven studies (n = 752) assessed the duration of analgesia, without significant difference (MD =- 1.55 min; 95% CI- 18.63, 15.53; I2 = 95%). However, six studies (n = 438) demonstrated that the addition of midazolam significantly prolonged motor block (MD = 15.48 min; 95% CI 3.97, 26.99; I2 = 94%). In obstetric surgeries, midazolam significantly extended both analgesia (MD = 39.73 min) and motor block (MD = 33.1 min). Fentanyl prolonged analgesia in non-obstetric surgeries (MD = - 16.90 min; 95% CI - 31.06, - 2.75). Risks of hypotension, bradycardia, and respiratory depression were similar, but fentanyl increased nausea, vomiting, shivering, and pruritus. Postoperative pain scores were comparable.
Conclusion: Fentanyl or midazolam added to bupivacaine show comparable sensory block durations. Midazolam prolongs motor block and analgesia in obstetric surgeries, while fentanyl extends analgesia in non-obstetric cases. Both show similar risks of hypotension, bradycardia, and respiratory depression, but fentanyl increases nausea, vomiting, shivering, and pruritus. There is no difference in postoperative pain scores. The findings need cautious interpretation due to considerable heterogeneity in the duration of sensory block, analgesia, and motor block, and unclear risk of bias. The low heterogeneity in safety outcomes supports a consistent safety profile.
Keywords: Adjuvant; Bupivacaine; Efficacy; Fentanyl; Meta-analysis; Midazolam; Safety; Spinal anesthesia.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests. Research registration: The review was registered in Research Registry with identifying number reviewregistry1918.
Figures


References
-
- Di Cianni S, Rossi M, Casati A, Cocco C, Fanelli G. Spinal anesthesia: an evergreen technique. Acta Biomedica-Ateneo Parmense. 2008;79(1):9. - PubMed
-
- Kumar V. Current indications for spinal anesthesia-a narrative review. Best Pract Res Clin Anaesthesiol. 2023;37(2):89–99. - PubMed
-
- Acosta JAH, Hidalgo FOZ, León MFC, Castañeda JJ. Complications in Spinal Anesthesia. 2024.
-
- Lee Y, Ngan Kee W, Muchhal K, Chan C. Randomized double-blind comparison of ropivacaine–fentanyl and bupivacaine–fentanyl for spinal anaesthesia for urological surgery. Acta Anaesthesiol Scand. 2005;49(10):1477–82. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
