

Development and Validation of a Nomogram to Predict Ventricular Fibrillation During Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction
- PMID: 40776936
- PMCID: PMC12326412
- DOI: 10.31083/RCM37301
Development and Validation of a Nomogram to Predict Ventricular Fibrillation During Percutaneous Coronary Intervention in Patients With Acute Myocardial Infarction
Abstract
Background: Ventricular fibrillation (VF) is a life-threatening complication of acute myocardial infarction (AMI), particularly in patients undergoing percutaneous coronary intervention (PCI). Early identification of high-risk patients is crucial for implementing preventive measures and improving outcomes.
Methods: This retrospective study analyzed clinical, laboratory, and angiographic data from 155 AMI patients to identify predictors of VF during PCI. Variable selection was performed using least absolute shrinkage and selection operator (LASSO) regression, elastic net regression, and random forest. Independent predictors were identified through multivariable logistic regression, and a nomogram was developed and validated to predict VF risk. Model performance was assessed using receiver operating characteristic (ROC) and calibration curves.
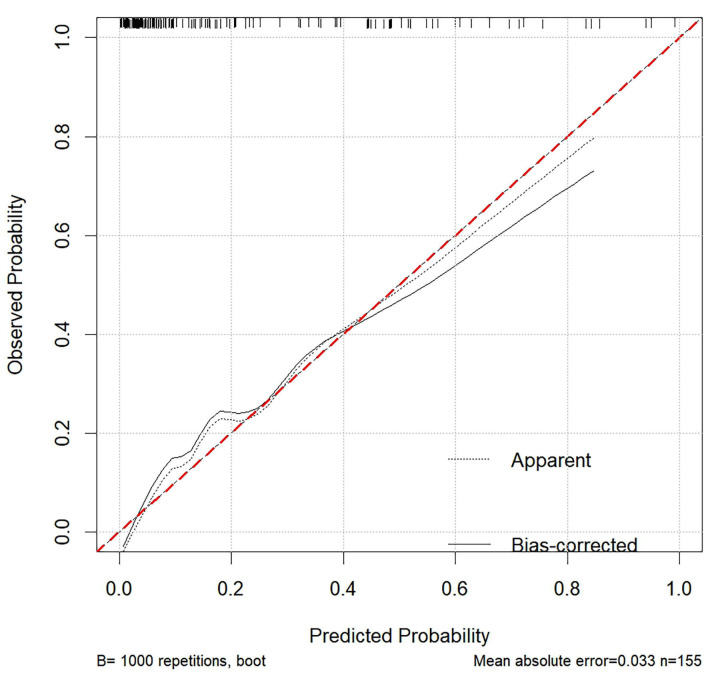
Results: Independent predictors of VF included diabetes (OR = 3.676 (1.365-10.668); p = 0.012), neutrophil-to-lymphocyte ratio (NLR) (odds ratio (OR) = 1.149 (1.053-1.265); p = 0.002), right coronary artery (RCA) intervention (OR = 3.185 (1.088-9.804); p = 0.037), Gensini score (OR = 1.020 (1.007-1.033); p = 0.003), and absence of beta blockers (OR = 0.168 (0.054-0.472); p = 0.001). The nomogram, incorporating these predictors, demonstrated a strong discriminative ability with an area under the ROC curve (AUC) of 0.882 (0.825-0.939) and good calibration (Hosmer-Lemeshow test, p = 0.769). The calibration curve showed a strong alignment between predicted probabilities and observed outcomes, with a mean absolute error of 0.033.
Conclusions: This study identified diabetes, NLR, RCA intervention, Gensini score, and absence of beta-blocker use as key predictors of VF during PCI in AMI patients. A nomogram incorporating these factors showed strong predictive performance, aiding clinicians in identifying high-risk patients for targeted preventive strategies.
Keywords: acute myocardial infarction (AMI); nomogram; percutaneous coronary intervention (PCI); ventricular fibrillation (VF).
Copyright: © 2025 The Author(s). Published by IMR Press.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Bougouin W, Marijon E, Puymirat E, Defaye P, Celermajer DS, Le Heuzey JY, et al. Incidence of sudden cardiac death after ventricular fibrillation complicating acute myocardial infarction: a 5-year cause-of-death analysis of the FAST-MI 2005 registry. European Heart Journal . 2014;35:116–122. doi: 10.1093/eurheartj/eht453. - DOI - PubMed
-
- Demidova MM, Carlson J, Erlinge D, Platonov PG. Predictors of ventricular fibrillation at reperfusion in patients with acute ST-elevation myocardial infarction treated by primary percutaneous coronary intervention. The American Journal of Cardiology . 2015;115:417–422. doi: 10.1016/j.amjcard.2014.11.025. - DOI - PubMed
-
- Kosmidou I, Embacher M, McAndrew T, Dizon JM, Mehran R, Ben-Yehuda O, et al. Early Ventricular Tachycardia or Fibrillation in Patients With ST Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention and Impact on Mortality and Stent Thrombosis (from the Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction Trial) The American Journal of Cardiology . 2017;120:1755–1760. doi: 10.1016/j.amjcard.2017.07.080. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
