

A rare dermatological manifestation of follicular spicules in a patient with multiple myeloma and end-stage renal disease on hemodialysis: A case report
- PMID: 40777564
- PMCID: PMC12329723
- DOI: 10.3892/etm.2025.12930
A rare dermatological manifestation of follicular spicules in a patient with multiple myeloma and end-stage renal disease on hemodialysis: A case report
Abstract
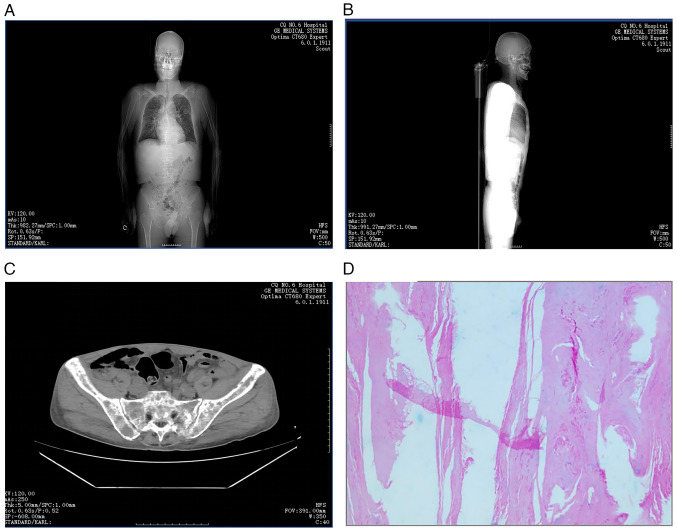
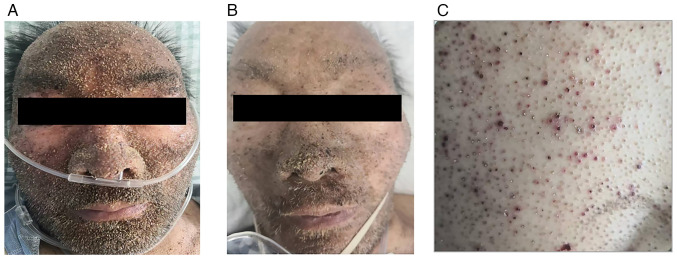
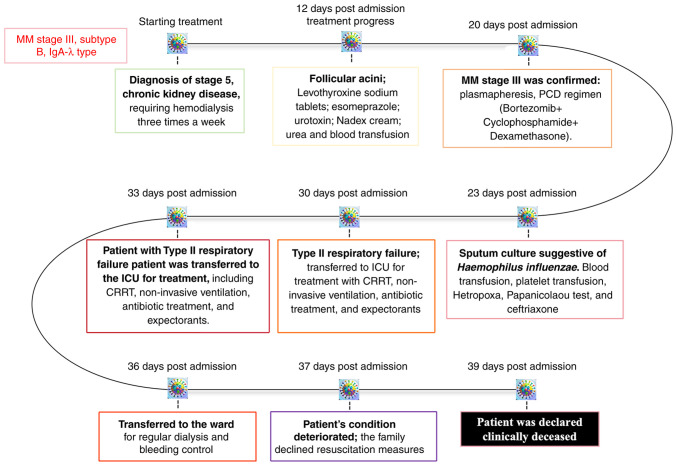
Multiple myeloma (MM) is a hematological malignancy characterized by the clonal expansion of malignant plasma cells within the bone marrow, leading to diverse systemic complications. While cutaneous manifestations of MM are uncommon, follicular spicules represent a highly specific but rare dermatological finding associated with MM. The present study presents the case of a 59-year-old man with MM who exhibited follicular acanthosis and hyperkeratosis as cutaneous indicators of the malignancy. The patient, with a history of stage 5 chronic kidney disease undergoing maintenance hemodialysis, was diagnosed with follicular spicules of MM (FSMM) through clinical evaluation and laboratory investigations. The present case highlights the clinical importance of recognizing rare cutaneous manifestations in MM, which can serve as critical diagnostic clues. Improved awareness of FSMM may facilitate a timely diagnosis and optimize patient management, ultimately contributing to improved clinical outcomes in this challenging population.
Keywords: chronic kidney disease; dermatological manifestations; end-stage renal disease; follicular acanthosis; follicular spicules; hemodialysis; hyperkeratosis; multiple myeloma.
Copyright: © 2025 Li et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Rudnicka L, Chrostowska S, Kamiński M, Waśkiel-Burnat A, Michalczyk A, Rakowska A, Olszewska M. The role of trichoscopy beyond hair and scalp diseases. A review. J Eur Acad Dermatol Venereol: Mar 15, 2023 (Epub ahead of print). - PubMed
-
- Michael A, Fuller T, Brogan S, Murphy MC. An intrathecal pump misadventure in two acts: An unrecognized partial pocket fill followed by an unusual withdrawal syndrome two months later. J Palliat Med: Jan 30, 2025 (Epub ahead of print). - PubMed
-
- Chang YC, Peng CY, Chi KY, Song J, Chang Y, Chiang CH, Gao W, Chiang CH. Cardiovascular outcomes and mortality in diabetic multiple myeloma patients initiated on proteasome inhibitors according to prior use of glucagon-like peptide 1 agonists. Eur J Prev Cardiol: Jan 29, 2025 (Epub ahead of print). - PubMed
Publication types
LinkOut - more resources
Full Text Sources