

Amaurosis fugax progressing to retinal artery occlusion with anterior migration of a retrobulbar embolus on orbital color Doppler imaging
- PMID: 40777925
- PMCID: PMC12329258
- DOI: 10.1016/j.ajoc.2025.102395
Amaurosis fugax progressing to retinal artery occlusion with anterior migration of a retrobulbar embolus on orbital color Doppler imaging
Abstract
Purpose: Orbital color Doppler imaging (CDI) is useful in the evaluation of sudden monocular vision loss, providing information on etiology which may guide management. We present two cases of amaurosis fugax progressing to retinal artery occlusion (RAO) associated with migration of a hyperechoic particle within the central retinal artery (CRA) and altered vascular dynamics found on CDI.
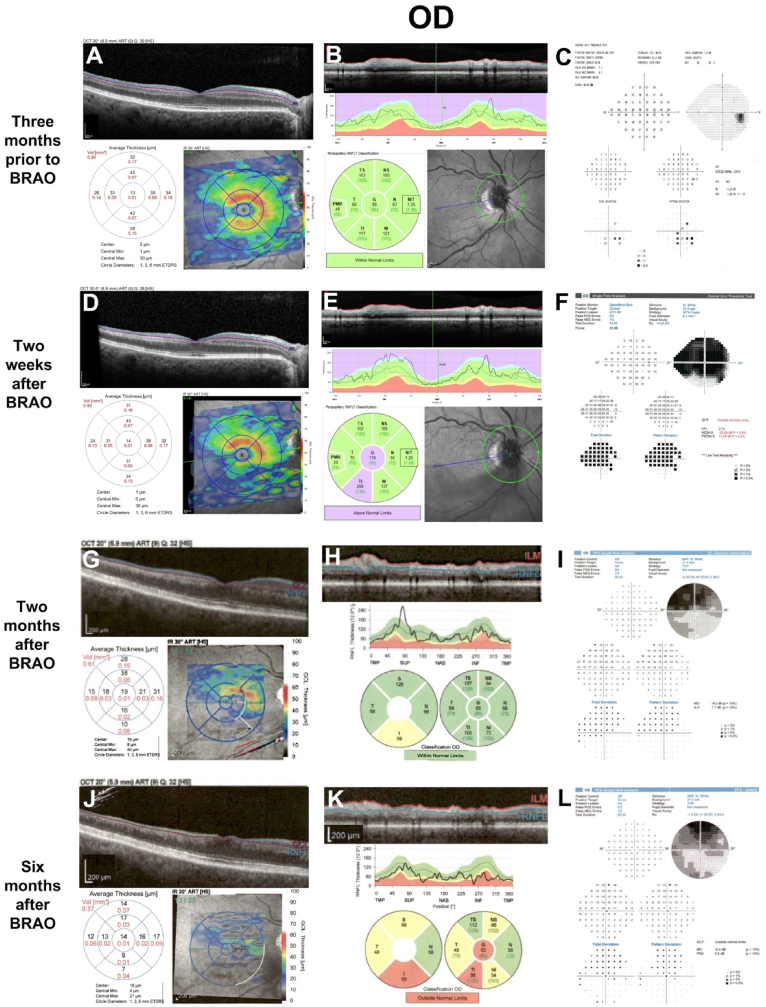
Observations: Both patients presented with amaurosis fugax, and CDI revealed a hyperechoic particle 2.8 mm from the optic nerve head in both patients. Patient 1 was found to have severe aortic stenosis and a thoracic aortic aneurysm and was managed with dual antiplatelet therapy (DAPT) while awaiting evaluation for cardiothoracic surgical repair. Ten days later, Patient 1 returned with a central RAO, and a repeat CDI showed a 1.0 mm anterior migration of the embolus with reduced CRA blood velocity and an increased resistivity index. Patient 2 was managed with DAPT and oral corticosteroids, but symptoms recurred during steroid tapering which necessitated a prolonged course of steroids. Systemic complications required reduction of steroid dosing, and the patient developed a branch RAO six months after initial presentation. Repeat CDI revealed a 0.9 mm anterior migration of the embolus, with increased CRA blood velocity and resistivity index. Systemic thrombolysis with tissue plasminogen activator and resumption of steroids did not result in visual improvement in Patient 2.
Conclusions and importance: The presence of a hyperechoic particle in the CRA on CDI can be seen with amaurosis fugax, and anterior migration with subsequent alterations in CDI parameters may correlate with clinical progression to embolic retinal ischemia. Visualization of an embolus may predict nonresponse to thrombolytic or anticoagulation-based treatment.
Keywords: Amaurosis fugax; Color Doppler imaging; Embolism; Orbital ultrasound; Retinal artery occlusion; Transient monocular vision loss.
© 2025 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


Similar articles
-
Carotid Artery Surgery.2025 May 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 May 2. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 28722976 Free Books & Documents.
-
Thrombolysis for acute ischaemic stroke.Cochrane Database Syst Rev. 2003;(3):CD000213. doi: 10.1002/14651858.CD000213. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2009 Oct 07;(4):CD000213. doi: 10.1002/14651858.CD000213.pub2. PMID: 12917889 Updated.
-
Anti-vascular endothelial growth factor for macular oedema secondary to branch retinal vein occlusion.Cochrane Database Syst Rev. 2013 Jan 31;(1):CD009510. doi: 10.1002/14651858.CD009510.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2020 Jul 7;7:CD009510. doi: 10.1002/14651858.CD009510.pub3. PMID: 23440840 Updated.
-
Prophylactic non-steroidal anti-inflammatory drugs for the prevention of macular oedema after cataract surgery.Cochrane Database Syst Rev. 2016 Nov 1;11(11):CD006683. doi: 10.1002/14651858.CD006683.pub3. Cochrane Database Syst Rev. 2016. PMID: 27801522 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
References
-
- Graefe A. Ueber Embolie der Arteria centralis retinae als Ursache plötzlicher Erblindung. Arch Ophthalmol. 1859;5:136–157.
Publication types
LinkOut - more resources
Full Text Sources
