

Early acetaminophen Use and 90-day mortality in ICU patients with ischemic stroke
- PMID: 40777988
- PMCID: PMC12328191
- DOI: 10.3389/fphar.2025.1622440
Early acetaminophen Use and 90-day mortality in ICU patients with ischemic stroke
Abstract
Introduction: The impact of acetaminophen on the prognosis of ischemic stroke patients admitted to intensive care units remains unclear. Although acetaminophen is commonly used for fever and pain management, its potential benefits beyond temperature control require further investigation.
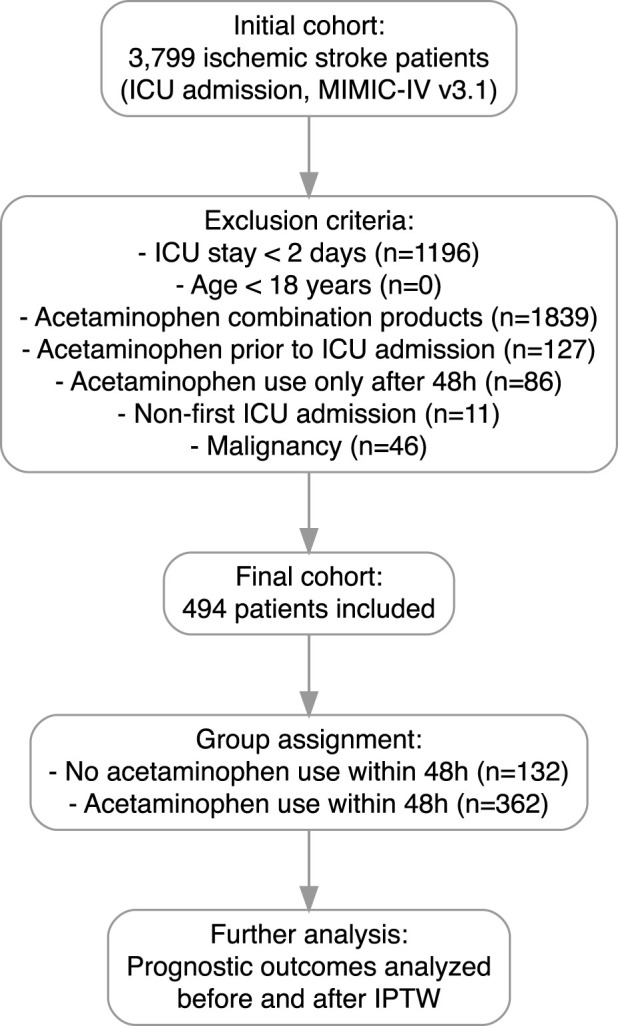
Methods: Using the MIMIC-IV database, we retrospectively identified 494 ICU-admitted ischemic stroke patients, of whom 362 (73.28%) received early acetaminophen treatment within 48 h after ICU admission. Patients were stratified based on acetaminophen exposure. Weighted Cox regression was applied after inverse probability of treatment weighting (IPTW) adjustment. Subgroup and sensitivity analyses were performed to assess the consistency of associations.
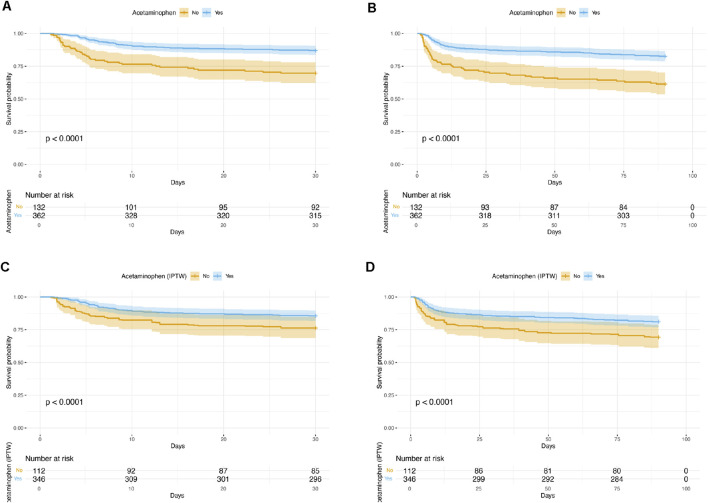
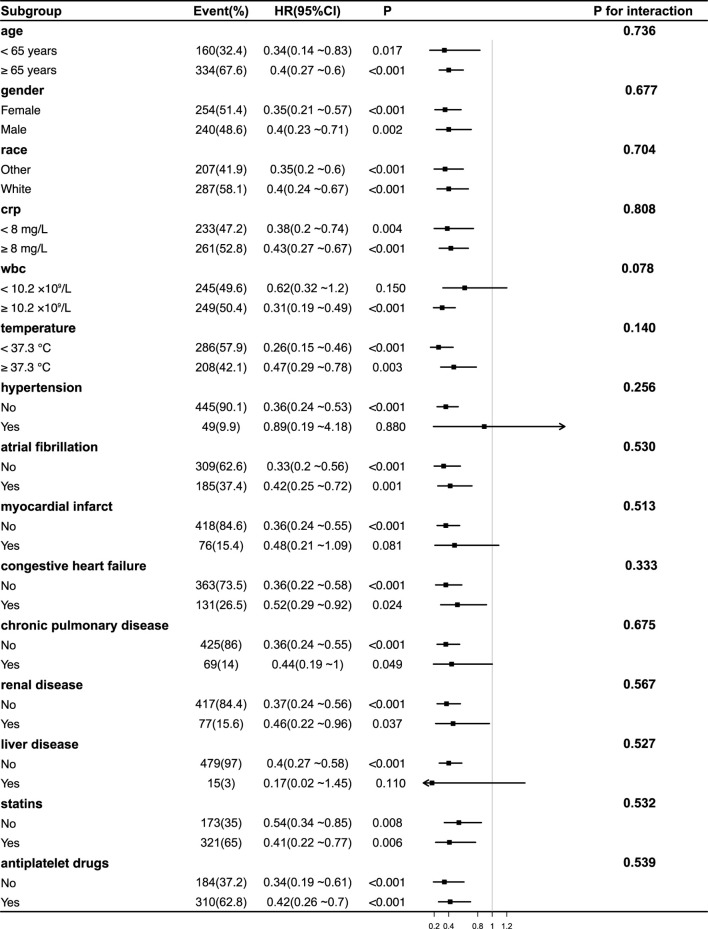
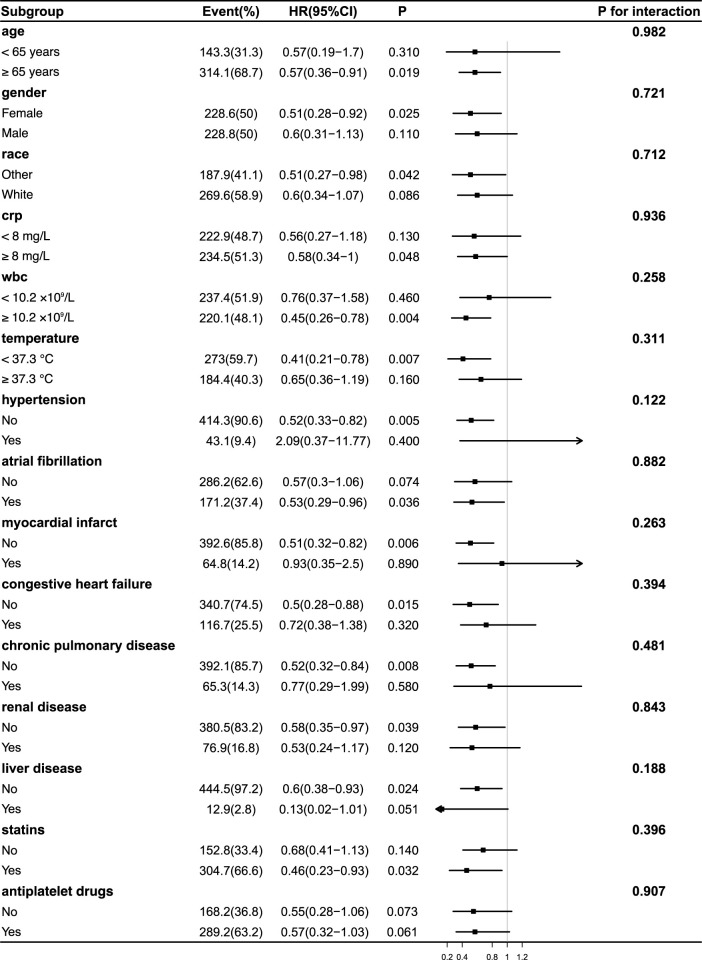
Results: After IPTW adjustment, early acetaminophen use was associated with reduced 30-day mortality (HR 0.54, 95% CI 0.31-0.94, p = 0.030), and reduced 90-day mortality (HR 0.53, 95% CI 0.32-0.87, p = 0.013). There were no significant differences in in-hospital mortality or hospital length of stay. Subgroup analyses revealed no significant interaction effects, suggesting a consistent association across different clinical strata.
Discussion: Early acetaminophen use may be associated with improved survival outcomes in critically ill ischemic stroke patients. These findings highlight the potential therapeutic value of acetaminophen beyond symptomatic treatment, warranting confirmation through prospective, multicenter randomized controlled trials.
Keywords: acetaminophen; intensive care units; inverse probability of treatment weighting; ischemic stroke; mortality.
Copyright © 2025 Piao, Zhang, Li, Jia and Cheng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Adams J. , H. P., Del Zoppo G., Alberts M. J., Bhatt D. L., Brass L., Furlan A., et al. (2007). Guidelines for the early management of adults with ischemic stroke: a guideline from the American heart association/american stroke association stroke council, clinical cardiology council, cardiovascular radiology and intervention council, and the atherosclerotic peripheral vascular disease and quality of care outcomes in research interdisciplinary working groups: the American academy of neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 38, 1655–1711. 10.1161/STROKEAHA.107.181486 - DOI - PubMed
-
- Cohen J. (2013). Statistical power analysis for the behavioral sciences. New York: routledge. 10.4324/9780203771587 - DOI
LinkOut - more resources
Full Text Sources