

Technique to Reduce Wound Size: The Double-Opposing Purse-String and Horizontal Continuous Closure Algorithm
- PMID: 40778241
- PMCID: PMC12331022
Technique to Reduce Wound Size: The Double-Opposing Purse-String and Horizontal Continuous Closure Algorithm
Abstract
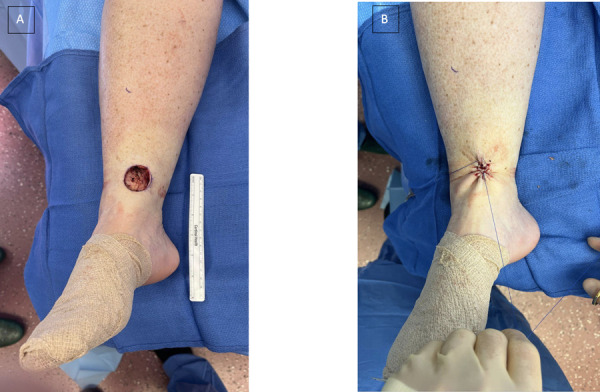
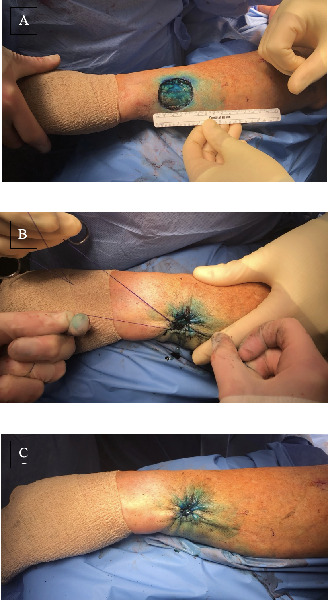
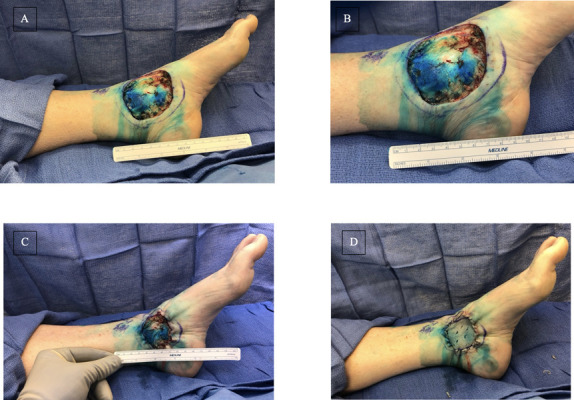
Background: Surgical reconstruction of complex wounds requires considerable planning to ensure optimal patient outcomes. A conservative approach utilizing the lower tiers of the reconstructive ladder is preferred, especially in patients with comorbidities lending to a higher risk of poor wound healing. A simplified, low-risk solution with a double-opposing purse-string suture (PSS) and horizontal continuous closure technique may be particularly helpful in reducing the need for more complex techniques of wound reconstruction in select patient populations.
Methods: A retrospective chart review was performed on all patients who underwent reconstruction with the double-opposing PSS technique (N = 57) by the senior author (B.J.W.) at the University of Louisville between 2019 and 2022.
Results: A total of 46 patients and 57 wounds underwent the double-opposing PSS and horizontal continuous closure technique as directed by the algorithm. The average defect size before and after was 61 and 12 cm2, respectively. A 2-tailed paired t test analysis was performed to explore the relationship between the pre- and post-closure defect size (P = .0003, t (44) = 3.9, 95% CI). A total of 21 wounds required a skin graft, meaning 63% of the wounds were successfully closed without the use of skin graft as a result of the double-opposing PSS technique. In addition, of those 21 wounds, the skin grafts, as well as the donor site sizes, were smaller.
Conclusions: This approach to wound closure demonstrates usefulness in reducing the size of or need for skin grafts in complex wound patients, particularly in those with comorbidities. The majority of patients underwent successful closure of their complex defects in various areas (eg, face, extremities) with this technique. Residual defects requiring skin graft allowed for a smaller graft and, thereby, donor site. Ultimately, this technique reduces the risk of complex complications by simplifying and reducing wound size.
Keywords: Complex Wound Closure; Purse-String; Skin Cancer; Skin Grafting; Surgical Technique; Wound Reconstruction.
© 2025 HMP Global. All Rights Reserved. Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of ePlasty or HMP Global, their employees, and affiliates.
Conflict of interest statement
Disclosures: The authors disclose no financial or nonficancial conflicts of interest.
Figures





References
-
- Coskunfirat OK, Chen HC, Spanio S, Tang YB. The safety of microvascular free tissue transfer in the elderly population. Plast Reconstr Surg. Mar 2005;115(3):771-5. doi:10.1097/01.prs.0000152424.91250.a5 10.1097/01.PRS.0000152424.91250.A5 - DOI - DOI - PubMed
-
- Janis JE, Harrison B. Wound healing: part I. Basic science. Plast Reconstr Surg. Feb 2014;133(2):199e-207e. doi:10.1097/01.prs.0000437224.02985.f9 10.1097/01.prs.0000437224.02985.f9 - DOI - DOI - PubMed
-
- Siana JE, Rex S, Gottrup F. The effect of cigarette smoking on wound healing. Scand J Plast Reconstr Surg Hand Surg. 1989;23(3):207-9. doi:10.3109/02844318909075119 - DOI - PubMed
-
- Anstead GM. Steroids, retinoids, and wound healing. Adv Wound Care. Oct 1998;11(6):277-85. - PubMed
-
- Ruberg RL. Role of nutrition in wound healing. Surg Clin North Am. Aug 1984;64(4):705-14. doi:10.1016/s0039-6109(16)43386-4 10.1016/S0039-6109(16)43386-4 - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources