

Non-invasive goal-directed fluid therapy with the pleth variability index (PVI): a systematic review and meta-analysis
- PMID: 40778974
- PMCID: PMC12474725
- DOI: 10.1007/s10877-025-01334-7
Non-invasive goal-directed fluid therapy with the pleth variability index (PVI): a systematic review and meta-analysis
Abstract
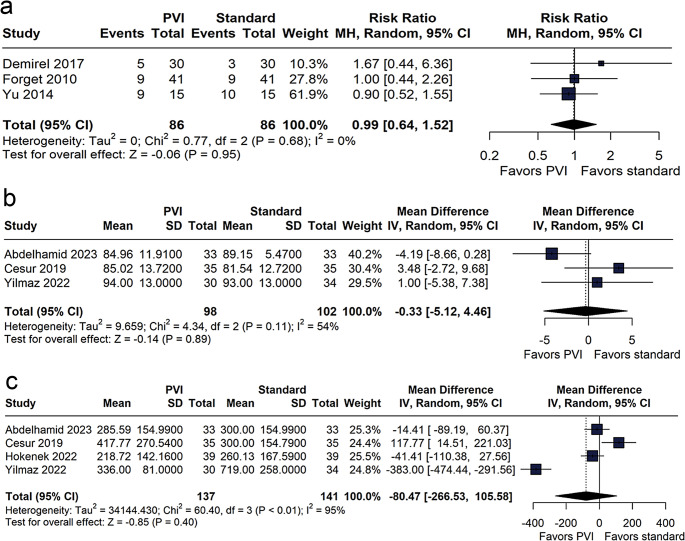
Optimal intraoperative fluid management is essential to improve surgical outcomes and reduce complications. The Pleth Variability Index (PVI), a dynamic and non-invasive indicator of fluid responsiveness, has been proposed as a tool for goal-directed fluid management. This systematic review and meta-analysis aimed to evaluate the effectiveness of PVI-guided fluid therapy compared to conventional fluid management (CFM) in non-cardiac surgeries. A comprehensive search of PubMed, Embase, and Cochrane databases up to January 2024 identified eligible studies. Primary outcomes included total intraoperative fluid volume and crystalloid administration. Secondary outcomes included hemodynamic parameters, renal function markers, acid-base balance, and hospital length of stay (LOS). Random-effects models were applied, and subgroup and sensitivity analyses were performed. Nine studies comprising 1,105 patients were included. Compared to conventional fluid management, PVI-guided therapy significantly reduced total fluid volume (mean difference [MD] - 761.23 mL; 95% CI - 1267.42 to - 255.03) and crystalloid administration (MD - 655.05 mL; 95% CI - 1096.48 to - 213.62), without significant differences in colloid use, urine output, norepinephrine requirement, arterial pressure, acid-base balance, or LOS. Subgroup analysis of abdominal surgeries confirmed the observed reduction in fluid volumes. PVI-guided fluid management allows for a more restrictive and individualized approach without compromising hemodynamic or metabolic stability. While the heterogeneity across studies limits generalizability, these findings support the clinical value of PVI as a non-invasive tool for perioperative fluid optimization, especially in settings where invasive monitoring is not feasible. Further trials are needed to evaluate its impact on long-term outcomes.
Keywords: Goal-directed fluid therapy; Meta-analysis; Perioperative fluid management; Pleth Variability Index (PVI); Systematic review.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures





References
-
- Cai J, Tang M, Wu H, Yuan J, Liang H, Wu X, Xing S, Yang X, Duan XD. Association of intraoperative hypotension and severe postoperative complications during non-cardiac surgery in adult patients: A systematic review and meta-analysis. Heliyon. 2023;9:e15997. 10.1016/j.heliyon.2023.e15997. - PMC - PubMed
-
- Walsh M, Devereaux PJ, Garg AX, Kurz A, Turan A, Rodseth RN, Cywinski J, Thabane L, Sessler DI. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology. 2013;119:507–15. 10.1097/ALN.0b013e3182a10e26. - PubMed
-
- Silva PL, Cruz FF, Fujisaki LC, Oliveira GP, Samary CS, Ornellas DS, Maron-Gutierrez T, Rocha NN, Goldenberg R, Garcia CS, Morales MM, Capelozzi VL, Gama de Abreu M, Pelosi P, Rocco PR. Hypervolemia induces and potentiates lung damage after recruitment maneuver in a model of sepsis-induced acute lung injury. Crit Care. 2010;14:R114. 10.1186/cc9063. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
