

The focal index: a quantitative approach to morphological sub-phenotyping of COVID-19 patients with acute respiratory distress syndrome: a pilot study
- PMID: 40779152
- PMCID: PMC12334779
- DOI: 10.1186/s40635-025-00794-0
The focal index: a quantitative approach to morphological sub-phenotyping of COVID-19 patients with acute respiratory distress syndrome: a pilot study
Abstract
Background: Acute respiratory distress syndrome (ARDS) is characterised by significant morphological heterogeneity. Morphological sub-phenotyping can potentially be used to personalise mechanical ventilation. Current methods to classify lung injury as focal or diffuse rely on subjective image interpretation, which risks misclassification and suboptimal treatment. This study aimed to investigate the morphological appearance features of lung injury objectively. The focal index, an objective quantitative tool, was introduced to assess focality in lung injury.
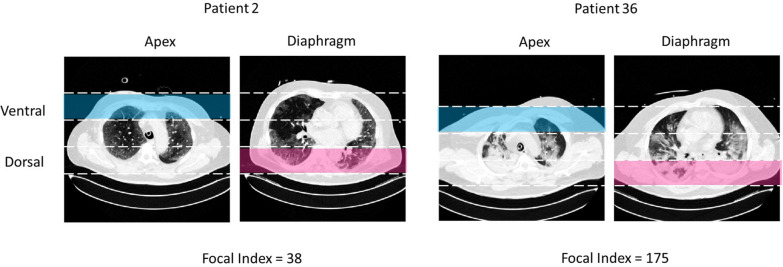
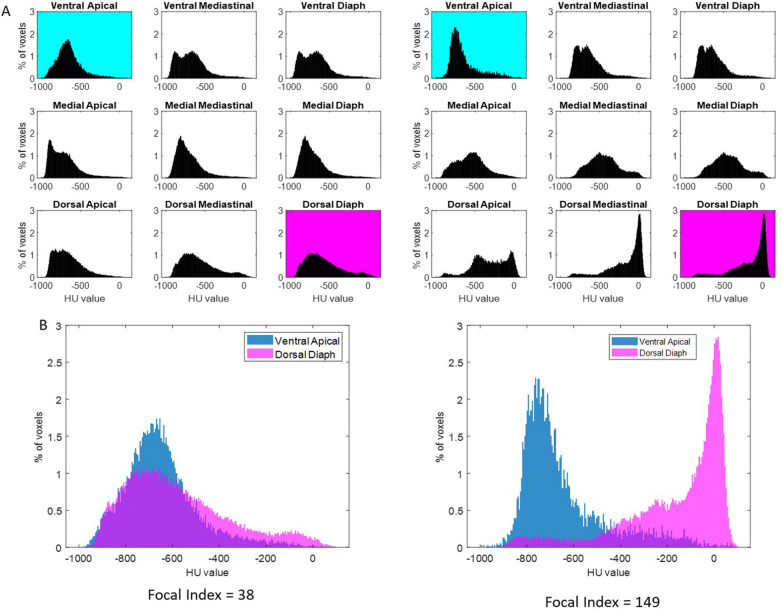
Methods: In this single-centre retrospective study, we included lung computed tomography (CT) scans from COVID-19 ARDS patients on invasive mechanical ventilation, classified as diffuse lung injury. CT data were analysed to extract regional Hounsfield Unit (HU) profiles across nine predefined lung areas. The focal index was derived by quantifying the non-overlapping area under HU distribution curves between the apical ventral and diaphragmatic dorsal regions. Correlations with lung weight, gas volume, and ventilatory settings were assessed. For validation, at least two experienced ICU consultants assessed the same images and determined whether ARDS was of a diffuse or focal type. The experts classified 36 out of 37 patients as diffuse ARDS, with substantial interobserver agreement (k = 0.65, 95% CI 0.02-1.00).
Results: The focal index demonstrated a wide range (25-175; mean 95.5 ± standard deviation 42.8), correlating significantly with the dorsal diaphragmatic non-aerated area (r = 0.67, p < 0.01) and with total gas volume (r = - 0.36, p = 0.03). There was no significant influence of ventilatory settings on the focal index.
Conclusions: The analysis suggested diffuse lung injury includes a spectrum of focality rather than a binary classification. The focal index provides an objective method to quantify the focality of lung injury in ARDS. Further studies are needed to validate the focal index across diverse ARDS aetiologies and establish its clinical application threshold for guiding personalised ventilation strategies.
Keywords: Acute respiratory distress syndrome; Lung imaging; Mechanical ventilation; Sub-phenotypes.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The Swedish National Ethical Review Authority (Dnr 2024-03697-01) approved this study. Consent for publication: Not applicable. Competing interests: All authors disclose any financial and personal conflicts of interest. MP serves on the Editorial Board for Intensive Care Medicine Experimental.
Figures




References
Grants and funding
LinkOut - more resources
Full Text Sources
