

Radiological features of chronic pulmonary histoplasmosis: Easily mistaken for tuberculosis
- PMID: 40779563
- PMCID: PMC12334033
- DOI: 10.1371/journal.pntd.0013219
Radiological features of chronic pulmonary histoplasmosis: Easily mistaken for tuberculosis
Abstract
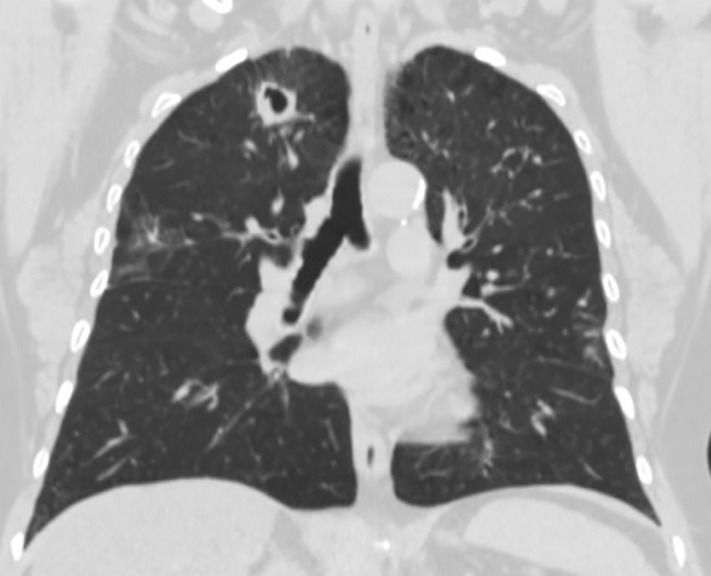
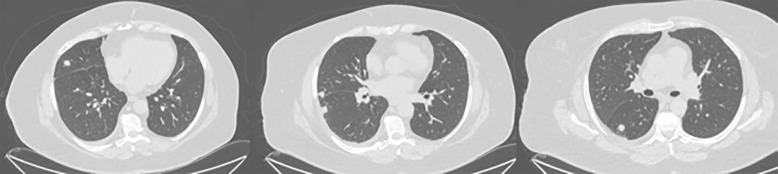
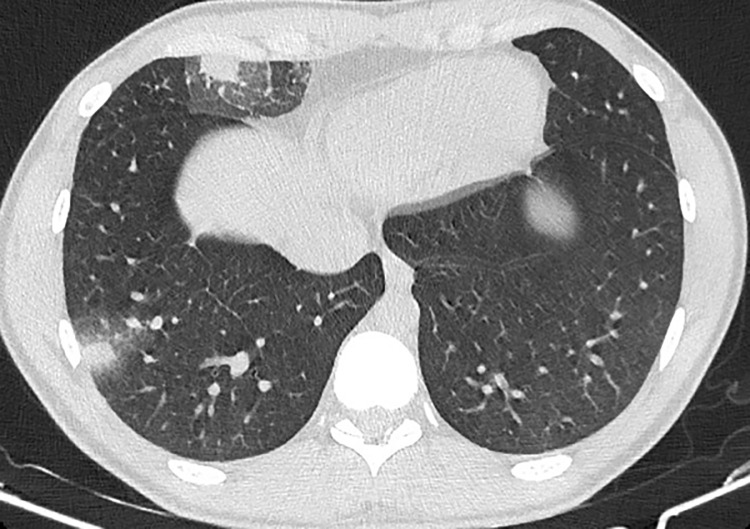
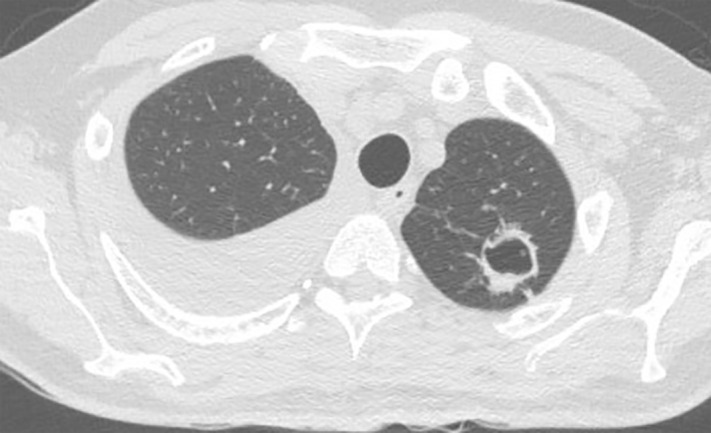
Histoplasma capsulatum var capsulatum is an endemic respiratory pathogen presenting in various forms including miliary histoplasmosis, acute and chronic pulmonary histoplasmosis, and acute or subacute disseminated disease. The differential diagnosis of chronic pulmonary histoplasmosis (CPH) is broad, encompassing bacterial, fungal and malignant aetiologies. PubMed was searched for relevant articles on the radiological characteristics of CPH and the most common differential diagnoses of tuberculosis and chronic pulmonary aspergillosis. The Fleischner Society Glossary of Terms for Thoracic Imaging was used to analyze the features. The contribution of culture, antibody and antigen and PCR to the diagnosis of CPH is summarized. Cavitation and pulmonary nodules are the most common features of CPH. Pleural effusion, pleural thickening, intrathoracic lymphadenopathy and bronchiectasis are not characteristic of CPH; uncommonly CPH can be complicated by an aspergilloma. Data on the radiologic features of CPH are derived primarily from the USA, Brazil, and China. CPH can be diagnosed by respiratory fungal culture (using extended culture times) or Histoplasma PCR (although data are scarce) and serum Histoplasma antigen and antibody. Data on bronchoscopy sampling for antigen are lacking. In patients with pulmonary cavitation without a confirmed diagnosis of tuberculosis or aspergillosis should be evaluated for CPH.
Copyright: © 2025 Denning et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
