

Optimizing Cardiovascular Risk Management in Primary Care Using a Personalized eCoach Solution Enhanced by an Artificial Intelligence-Driven Clinical Prediction Model: Protocol from the Coronary Artery Disease Risk Estimation and Early Detection Consortium
- PMID: 40779763
- PMCID: PMC12374134
- DOI: 10.2196/66068
Optimizing Cardiovascular Risk Management in Primary Care Using a Personalized eCoach Solution Enhanced by an Artificial Intelligence-Driven Clinical Prediction Model: Protocol from the Coronary Artery Disease Risk Estimation and Early Detection Consortium
Abstract
Background: Atherosclerotic cardiovascular disease poses a heavy burden on the population's health and health care costs. Identifying apparently healthy individuals at risk of developing cardiovascular diseases using clinical prediction models raises awareness, facilitates shared decision-making, and supports tailored management of disease prevention. In the CARRIER project, a personalized cardiovascular risk management (CVRM) eCoach approach is cocreated, in which identified individuals receive education, guidance, and monitoring to prevent atherosclerotic cardiovascular disease through existing interventions. In this approach, an artificial intelligence-driven clinical prediction model calculates the 10-year risk for atherosclerotic cardiovascular disease, which supports informed decision-making.
Objective: This study aims to assess the effectiveness of our CVRM eCoach approach through a 10-year risk calculation of atherosclerotic cardiovascular disease, including risk factors contributing to this risk.
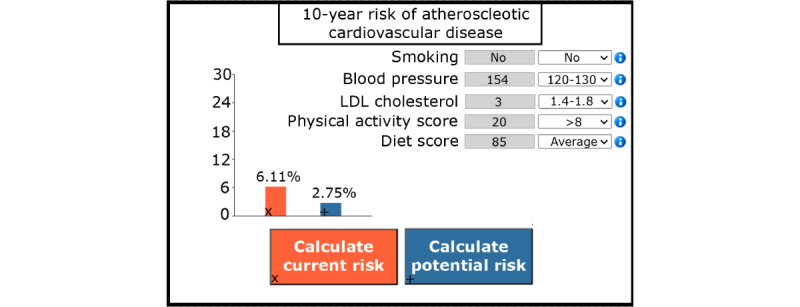
Methods: This pretest-posttest interventional study provides the CVRM eCoach approach for 6 months to 100 apparently healthy individuals eligible for CVRM. The CVRM eCoach approach is a multicomponent eHealth solution, including a clinical prediction under intervention model that not only calculates the 10-year risk of cardiovascular disease through conventional risk factors (smoking, blood pressure, and lipid profile) and individual characteristics (age, gender, socioeconomic status, physical activity, and diet) but also calculates how the risk changes after hypothetical lifestyle or medical interventions. The CVRM eCoach approach includes features that encourage behavior change. Most of these features include goal setting, decision cards to help decide on an intervention, intervention monitoring, remote communication, and education, all accessible from one dashboard. A practice nurse or physician consults the individuals after risk calculation with the clinical prediction model and uses behavior change features, such as the decision cards, to support shared decision-making. Data are primarily collected via the eCoach, after which the 10-year risk for atherosclerotic cardiovascular disease and its components are analyzed using paired-sample analyses.
Results: Recruitment began in March 2024 and will continue until 100 participants have been recruited, which is expected in 2025.
Conclusions: We anticipate that our CVRM eCoach approach will be valuable in the primary prevention setting. During the crucial initial first months of habit formation, factors such as education, regular check-ups via the eCoach, and clear risk communication could support individuals in sustaining their medical or lifestyle interventions. We hypothesize that there will be a slight to moderate reduction in the 10-year risk of atherosclerotic cardiovascular disease, which over time will lead to significant health improvements on a larger scale.
Trial registration: CCMO NL84584.096.23; https://onderzoekmetmensen.nl/nl/trial/56578.
Keywords: AI-driven; artificial intelligence; atherosclerosis; atherosclerotic cardiovascular disease; cardiovascular; cardiovascular disease; cardiovascular risk management; clinical prediction model; costs; digital health; disease management; eCoach; effectiveness; medical informatics; prediction model; primary care; risk management.
©Rutger van Mierlo, Bart Scheenstra, Joost Verbeek, Anke Bruninx, Petros Kalendralis, Inigo Bermejo, Andre Dekker, Arnoud van 't Hof, Marieke Spreeuwenberg, Laura Hochstenbach. Originally published in JMIR Research Protocols (https://www.researchprotocols.org), 08.08.2025.
Conflict of interest statement
Conflicts of Interest: AD is the founder, a stockholder, and an employee of Medical Data Works B.V. AvH received unrestricted grants from Abbott Vascular, Medtronic, Boehringer Ingelheim.
Figures




References
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R, Prospective Studies Collaboration Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. doi: 10.1016/s0140-6736(02)11911-8.S0140673602119118 - DOI - PubMed
-
- Prospective Studies Collaboration. Lewington S, Whitlock G, Clarke R, Sherliker P, Emberson J, Halsey J, Qizilbash N, Peto R, Collins R. Blood cholesterol and vascular mortality by age, sex, and blood pressure: a meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet. 2007;370(9602):1829–1839. doi: 10.1016/S0140-6736(07)61778-4.S0140-6736(07)61778-4 - DOI - PubMed
-
- Jha P, Ramasundarahettige C, Landsman V, Rostron B, Thun M, Anderson RN, McAfee T, Peto R. 21st-century hazards of smoking and benefits of cessation in the United States. N Engl J Med. 2013;368(4):341–350. doi: 10.1056/NEJMsa1211128. https://core.ac.uk/reader/82550963?utm_source=linkout - DOI - PubMed
-
- Schultz WM, Kelli HM, Lisko JC, Varghese T, Shen J, Sandesara P, Quyyumi AA, Taylor HA, Gulati M, Harold JG, Mieres JH, Ferdinand KC, Mensah GA, Sperling LS. Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation. 2018;137(20):2166–2178. doi: 10.1161/CIRCULATIONAHA.117.029652. https://europepmc.org/abstract/MED/29760227 CIRCULATIONAHA.117.029652 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
