

Combined TAVR and Ventricular Tachycardia Ablation for VT Storm With Severe Aortic Stenosis
- PMID: 40780796
- PMCID: PMC12426516
- DOI: 10.1016/j.jaccas.2025.104655
Combined TAVR and Ventricular Tachycardia Ablation for VT Storm With Severe Aortic Stenosis
Abstract
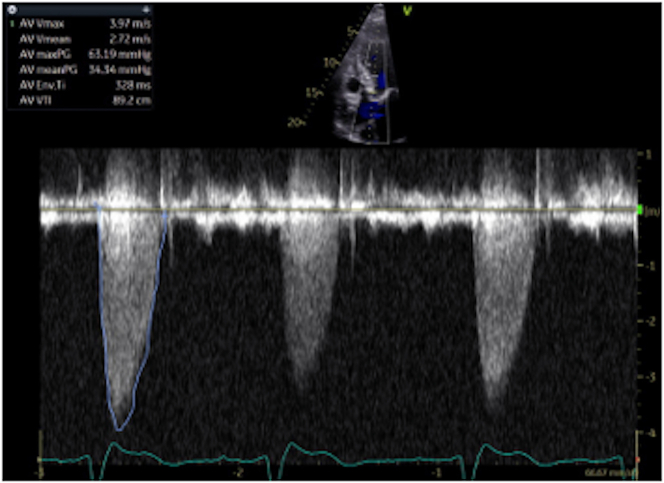
Objective: To describe the feasibility and clinical considerations of a simultaneous transcatheter aortic valve replacement (TAVR) and ventricular tachycardia (VT) ablation in a critically ill patient with severe aortic stenosis and VT storm.
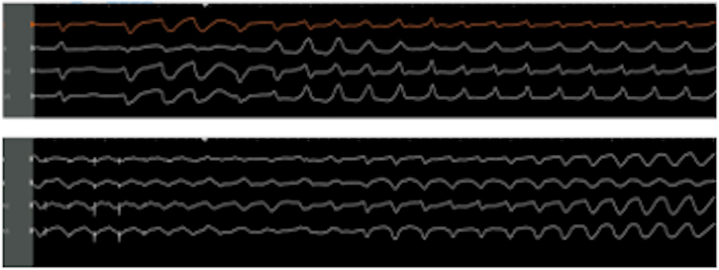
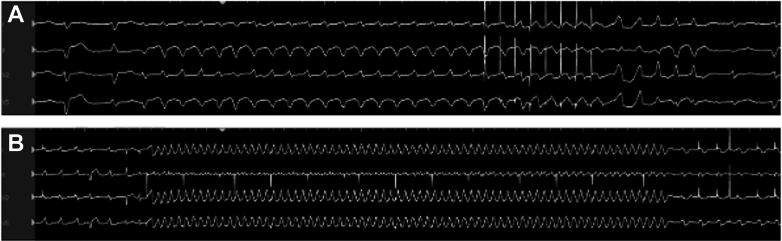
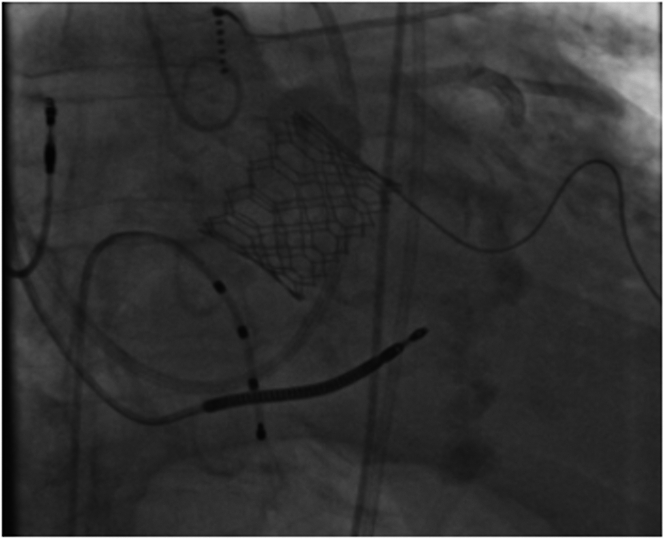
Key steps: Preprocedural planning involved both electrophysiology and structural teams present. Transfemoral TAVR was performed using a Sapien S3 valve (Edwards Lifesciences) under general anesthesia with both transesophageal and transthoracic echocardiography guidance. While crossing the aortic valve into the left ventricle, VT occurred and was promptly cardioverted.We then transitioned to ablation of VTs, targeting their origin in the left ventricular scar. After the procedure, we monitored for recurrence of VT and potential device upgrade for heart block. Potential Pitfalls: Issues that can arise include hemodynamic instability during valve crossing and rapid pacing, risk of complete heart block, reinducibility of VT after valve implantation, and prolonged procedure time, which requires careful anesthetic and electrophysiologic planning.
Take-home messages: Combined TAVR and VT ablation is feasible and can effectively treat 2 life-threatening problems in high-risk patients. A team-based, individualized approach is essential for procedural success.
Keywords: ablation; aortic valve; stenosis; ventricular tachycardia.
Copyright © 2025 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Stevenson has received speaking honoria from Abbott, Johnson & Johnson, Biotronik, Boston Scientific, and Mediasphere; and research funding from Adagio and Varian Medical Systems. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



References
-
- Otto C., Nishimura R., et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2021;77(4):e25–e197. doi: 10.1016/j.jacc.2020.11.018. - DOI - PubMed
-
- Sorgato A., Faggiano P., Aurigemma G.P., Rusconi C., Gaasch W.H. Ventricular arrhythmias in adult aortic stenosis: prevalence, mechanisms, and clinical relevance. Chest. 1998;113(2):482–491. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
