

Artificial intelligence-driven decision support for patients with acute respiratory failure: a scoping review
- PMID: 40781197
- PMCID: PMC12334380
- DOI: 10.1186/s40635-025-00791-3
Artificial intelligence-driven decision support for patients with acute respiratory failure: a scoping review
Abstract
Background: Artificial intelligence (AI) has emerged as a promising tool for decision support in managing acute respiratory failure, yet its real-world clinical impact remains unclear. This scoping review identifies clinically validated AI-driven tools in this domain, focusing on the reporting of key evaluation quality measures that are a prerequisite for broader deployment.
Eligibility criteria: Studies were included if they compared a clinical, human factors, or health systems-related outcome of an AI-driven intervention to a control group in adult patients with acute respiratory failure. Studies were excluded if they lacked a machine learning model, compared models trained on the same dataset, assessed only model performance, or evaluated models in simulated settings. A systematic literature search was conducted in PubMed, CINAHL, and EmBase, from inception until January 2025. Each abstract was independently screened by two reviewers. One reviewer extracted data and performed quality assessment, following the DECIDE-AI framework for early-stage clinical evaluation of AI-based decision support systems.
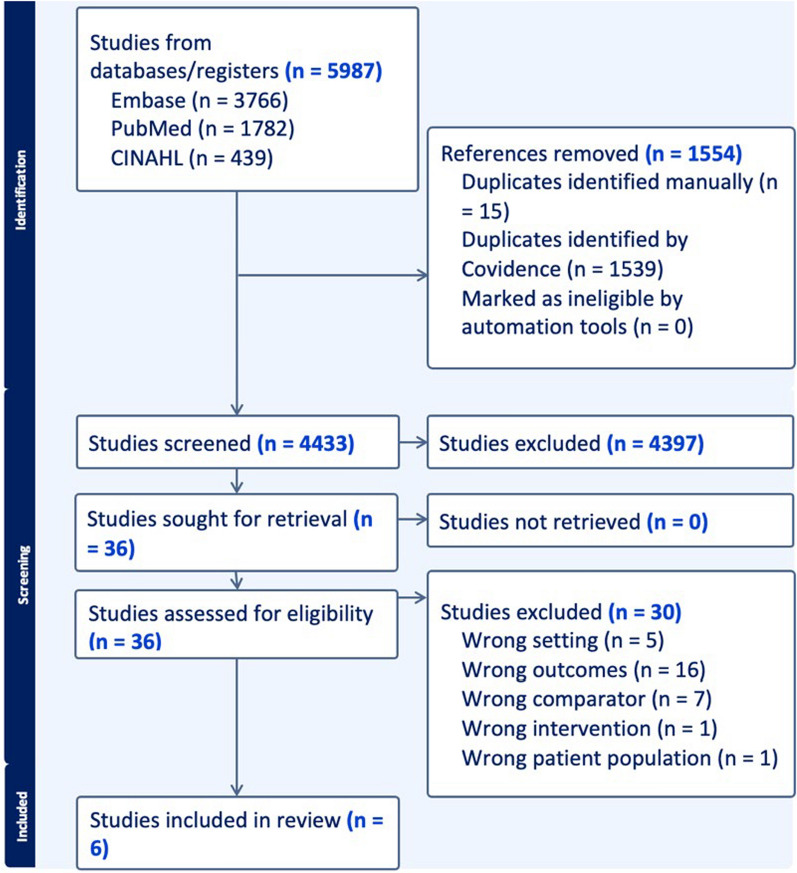
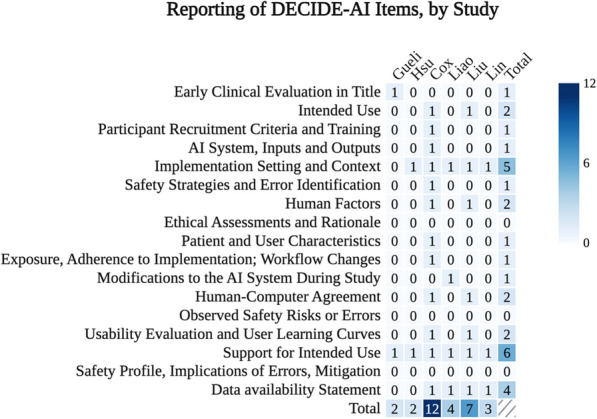
Results: Of 5,987 citations, six studies met eligibility. The studies, conducted between 2012 and 2024 in Taiwan, Italy, and the U.S., included 40-2,536 patients. Four studies (67%) focused on predicting weaning from mechanical ventilation. Three (50%) of the studies demonstrated a statistically significant and clinically meaningful outcome. Studies met a median of 3.5 (IQR: 2.25-6.25) of the 17 DECIDE-AI criteria. None reported AI-related errors, malfunctions, or algorithmic fairness considerations. Only one study (17%) described user characteristics and adherence, while two (33%) assessed human-computer agreement and usability.
Conclusions: Our review identified six studies evaluating AI-driven decision support tools for acute respiratory failure, with most focusing on predicting weaning from mechanical ventilation. However, methodological rigor for early clinical evaluation was inconsistent, with studies meeting few of the DECIDE-AI criteria. Notably, critical aspects such as error reporting, algorithmic fairness, and user adherence were largely unaddressed. Further high-quality assessments of reliability, usability, and real-world implementation are essential to realize the potential of these tools to transform patient care.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: N/A as this is a scoping review article. Consent for publication: N/A, no individual person’s data are included. Competing interests: Dr. Malhotra is funded by NIH and reports income from Eli Lilly, Zoll, Livanova, and Powell Mansfield. He is co-founder of Healcisio, a small startup from UCSD related to predictive analytics.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
-
AI in Medical Questionnaires: Scoping Review.J Med Internet Res. 2025 Jun 23;27:e72398. doi: 10.2196/72398. J Med Internet Res. 2025. PMID: 40549427 Free PMC article.
-
Education support services for improving school engagement and academic performance of children and adolescents with a chronic health condition.Cochrane Database Syst Rev. 2023 Feb 8;2(2):CD011538. doi: 10.1002/14651858.CD011538.pub2. Cochrane Database Syst Rev. 2023. PMID: 36752365 Free PMC article.
-
Effects of consumers and health providers working in partnership on health services planning, delivery and evaluation.Cochrane Database Syst Rev. 2021 Sep 15;9(9):CD013373. doi: 10.1002/14651858.CD013373.pub2. Cochrane Database Syst Rev. 2021. PMID: 34523117 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
