

Trends and disparities in heart failure mortality with and without chronic kidney disease in a nationwide retrospective analysis
- PMID: 40781259
- PMCID: PMC12334672
- DOI: 10.1038/s41598-025-04056-7
Trends and disparities in heart failure mortality with and without chronic kidney disease in a nationwide retrospective analysis
Abstract
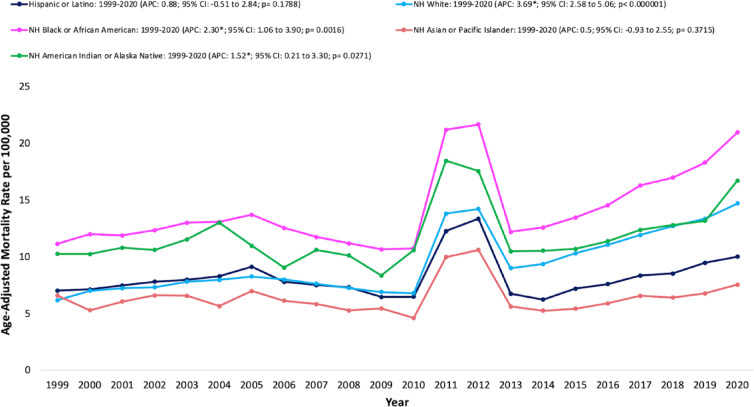
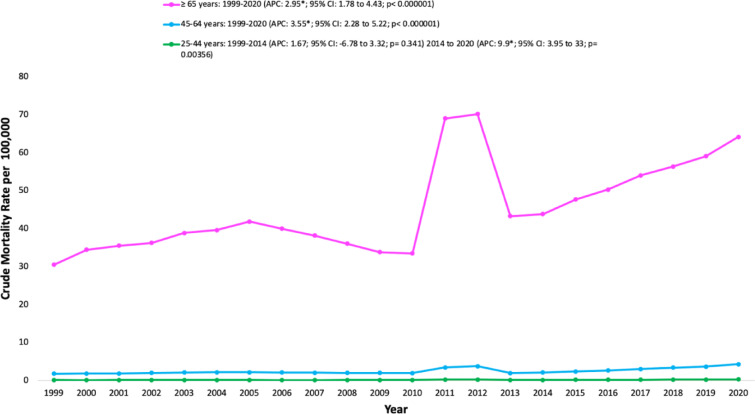
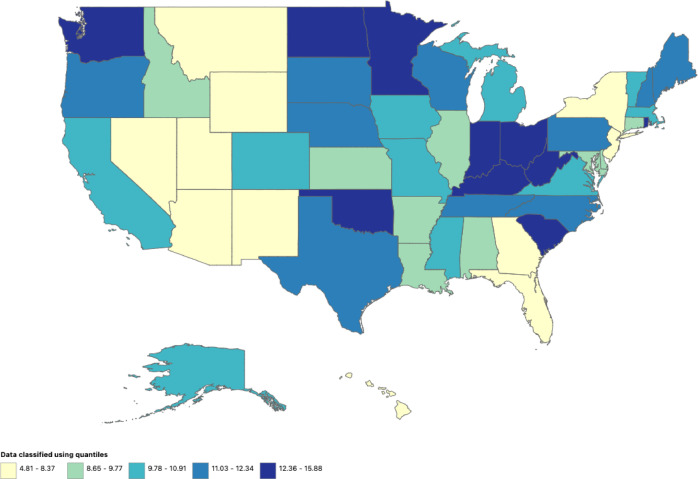
Chronic kidney disease (CKD) is a significant global contributor to morbidity and mortality, with many CKD patients developing heart failure (HF), leading to worsened outcomes. However, limited research has examined temporal trends and disparities in patients with concurrent HF and CKD. Using the Centers for Disease Control and Prevention's Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER) database, we analyzed concurrent HF and CKD-related deaths among adults aged ≥ 25 years. Mortality rates were stratified by age, sex, race/ethnicity, urbanization, and region. Age-adjusted mortality rates (AAMRs) and crude mortality rates (CMRs) per 100,000 were calculated. Trends were assessed using annual percentage changes (APCs) and average APC differences via Joinpoint Regression software. Statistical significance was defined as p < 0.05. From 1999 to 2020, the AAMR increased from 6.74 in 1999 to 8.88 in 2005 (APC 3.90%, 95% CI: 2.83-5.07, p < 0.001), declined to 7.18 in 2010 (APC - 4.15%, 95% CI: -5.78 to -3.03, p < 0.001), then rose sharply to 14.78 in 2020 (APC 7.46%, 95% CI: 7.05-7.87, p < 0.001). Males exhibited a higher AAMR (13.46) than females (7.9). Non-Hispanic (NH) Black individuals had the highest AAMR (15.05). Mortality was highest in the Midwest (AAMR 11.77) and among rural populations (AAMR 11.77) compared to urban residents. Mortality trends for concurrent HF and CKD surpassed those for HF or CKD alone. Concurrent HF and CKD-related mortality has increased across all demographic groups, with the highest risks observed in men, NH Black individuals, and rural populations. These findings underscore the need for targeted interventions to address these disparities.
Keywords: Chronic kidney disease; Epidemiology; Heart failure; Mortality trends.; Public health; United States.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Competing interests: The authors declare no competing interests.
Figures





References
-
- CDC & Chronic Kidney, D. [cited 2024 Dec 1]. Chronic Kidney Disease Basics. (2024). Available from: https://www.cdc.gov/kidney-disease/about/index.html
-
- CDC & Chronic Kidney, D. [cited 2024 Dec 1]. Risk Factors for Chronic Kidney Disease. (2024). Available from: https://www.cdc.gov/kidney-disease/risk-factors/index.html
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
