

Home-based digital counselling by frontline community workers for anxiety and depression symptoms in rural Sindh, Pakistan: the mPareshan intervention
- PMID: 40781292
- PMCID: PMC12333263
- DOI: 10.1186/s12889-025-23665-5
Home-based digital counselling by frontline community workers for anxiety and depression symptoms in rural Sindh, Pakistan: the mPareshan intervention
Abstract
Background: There is limited evidence that interventions for improving mental well-being can be integrated sustainably into primary health care in Pakistan. We piloted 'mPareshan digital intervention' locally, adapted from WHO mhGAP and delivered by trained and supervised women lay workers to learn if it was feasible and possibly effective in reducing anxiety and depression prior to proposing implementation on a larger scale.
Methods: Using Generalized Anxiety Disorder-7 (GAD-7) and Patient Health Questionnaire-9 (PHQ-9), a baseline household survey was conducted by independent data collectors to measure anxiety and depression. We trained 72 government Lady Health Workers (LHWs) and Lady Health Supervisors (LHSs) in District Badin, Sindh to screen and counsel adult men and women (> 18 years) with mild and moderate symptoms of anxiety and depression. Supervised by LHSs, these screen positive participants (SPs) received 6 counselling sessions by LHWs through the mPareshan app during their routine household visits. The app had interactive audio/video psychoeducation features. Severe anxiety and depression cases were referred to nearest available mental health service.
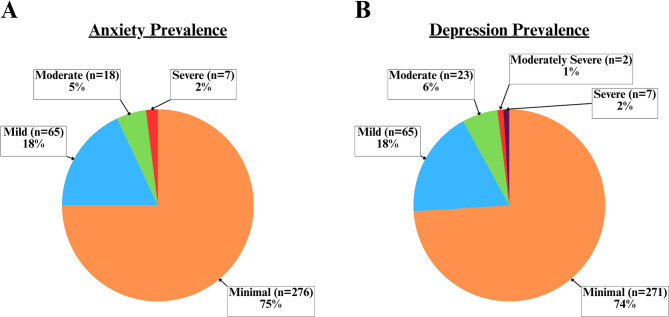
Results: Of the 366 individuals surveyed at baseline, 75% had minimal anxiety, 23% had mild to moderate anxiety, and 2% had severe anxiety. 74% had minimal depression, 24% had mild to moderate depression, and 2% had moderately severe to severe depression. 98 participants (53 men and 45 women, mean age 43.2 years) screened positive for mild and moderate anxiety and/or depression and were eligible for the mPareshan intervention. Six SPs did not complete the intervention for various reasons. Of the 92 SPs who completed all 6 monthly counselling sessions, their mean PHQ-9 score declined from 7.5 (SD 3.1) to 2.6 (SD 2.2) after intervention. Mean GAD-7 score fell from 6.6 (SD 3.0) to 2.1 (SD 2.2) after 6 sessions. No significant association between sociodemographic variables (age, gender, education, and income levels) and anxiety and depression scores was noted.
Conclusion: Preliminary evidence suggests meaningful reduction in anxiety and depression using this locally adapted digital counselling intervention delivered by lay health workers in a rural setting of Sindh, Pakistan. An appropriately powered randomized control trial is needed to test effectiveness of this task-shifting model.
Trial registration: Registered as non-randomized, pretest-posttest, feasibility trial on 14/07/2022 with Registration number ACTRN12622000989741 at the Australian New Zealand Clinical Trial Registry ( https://www.anzctr.org.au/Default.aspx ).
Keywords: Anxiety; Depression; Digital counselling; Lady health workers; Mental health; Primary health care; Task-shifting.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was approved by the Ethical Review Committee of Aga Khan University (ERC#2021-6570-20015). The study adheres to the tenets of the Declaration of Helsinki. All study participants (both for baseline and intervention) provided written informed consent which was given to them in their local language. Illiterate participants provided verbal consent, and their thumb impression were taken along with a witness present to note their consent. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures


Similar articles
-
Technology-Assisted Mental Health Intervention Delivered by Frontline Workers at Community Doorsteps for Reducing Anxiety and Depression in Rural Pakistan: Protocol for the mPareshan Mixed Methods Implementation Trial.JMIR Res Protoc. 2024 Jul 23;13:e54272. doi: 10.2196/54272. JMIR Res Protoc. 2024. PMID: 39042878 Free PMC article.
-
Psychological therapies for women who experience intimate partner violence.Cochrane Database Syst Rev. 2020 Jul 1;7(7):CD013017. doi: 10.1002/14651858.CD013017.pub2. Cochrane Database Syst Rev. 2020. PMID: 32608505 Free PMC article.
-
Investigation and analysis of mental health status of the older adult in western rural areas.Front Public Health. 2025 Jul 16;13:1612600. doi: 10.3389/fpubh.2025.1612600. eCollection 2025. Front Public Health. 2025. PMID: 40740371 Free PMC article.
-
Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: qualitative evidence synthesis.Cochrane Database Syst Rev. 2013 Oct 8;2013(10):CD010414. doi: 10.1002/14651858.CD010414.pub2. Cochrane Database Syst Rev. 2013. PMID: 24101553 Free PMC article.
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
References
-
- World Health Organization. World mental health report: transforming mental health for all. 2022.
-
- Javed A, Lee C, Zakaria H, Buenaventura RD, Cetkovich-Bakmas M, Duailibi K, et al. Reducing the stigma of mental health disorders with a focus on low- and middle-income countries. Asian J Psychiatry. 2021;58:102601. 10.1016/j.ajp.2021.102601. - PubMed
-
- World Health Organization. COVID-19 pandemic triggers 25% increase in prevalence of anxiety and depression worldwide. World Health Organization; 2022 Mar. https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-i....
MeSH terms
Grants and funding
- Grant Brain & Mind-FR-11E-mPareshan App 83000/Brain and Mind Institute, Aga Khan University
- Grant Brain & Mind-FR-11E-mPareshan App 83000/Brain and Mind Institute, Aga Khan University
- Grant Brain & Mind-FR-11E-mPareshan App 83000/Brain and Mind Institute, Aga Khan University
- Grant Brain & Mind-FR-11E-mPareshan App 83000/Brain and Mind Institute, Aga Khan University
- Grant Brain & Mind-FR-11E-mPareshan App 83000/Brain and Mind Institute, Aga Khan University
LinkOut - more resources
Full Text Sources
Medical
