

Cost-effectiveness of rapid, ICU-based, syndromic PCR in hospital-acquired pneumonia: analysis of the INHALE WP3 multi-centre RCT
- PMID: 40781331
- PMCID: PMC12333181
- DOI: 10.1186/s13054-025-05428-1
Cost-effectiveness of rapid, ICU-based, syndromic PCR in hospital-acquired pneumonia: analysis of the INHALE WP3 multi-centre RCT
Erratum in
-
Correction: Cost-effectiveness of rapid, ICU-based, syndromic PCR in hospital-acquired pneumonia: analysis of the INHALE WP3 multi-centre RCT.Crit Care. 2025 Sep 16;29(1):396. doi: 10.1186/s13054-025-05645-8. Crit Care. 2025. PMID: 40958116 Free PMC article. No abstract available.
Abstract
Background: Hospital-acquired and ventilator-associated pneumonia (HAP and VAP) are pneumonias arising > 48 h after admission or intubation respectively. Conventionally, HAP/VAP patients are given broad-spectrum empiric antibiotics at clinical diagnosis, refined after 48-72 h, once microbiology results become available. Molecular tests offer swifter results, potentially improving patient care. To investigate whether this potential is realisable, we conducted a pragmatic multi-centre RCT ('INHALE WP3') of rapid, syndromic polymerase chain reaction (PCR) in ICU HAP/VAP compared with standard of care. As the use of molecular tests impact on hospital resources, it is important to consider their potential value-for-money to make fully informed decisions. Consequently, INHALE WP3 included an economic evaluation, presented here. Its aim was to estimate the cost-effectiveness of an in-ICU PCR (bioMérieux BioFire FilmArray Pneumonia Panel) in HAP/VAP, informing whether to implement such technology in routine NHS care.
Methods: We collected data on patient resource use and costs. These data were combined with INHALE WP3's two primary outcome measures: antibiotic stewardship at 24 h and clinical cure at 14 days. Cost-effectiveness analyses were carried out using regression models adjusting for site. Sensitivity analyses explored assumptions and sub-group analyses explored differential impacts.
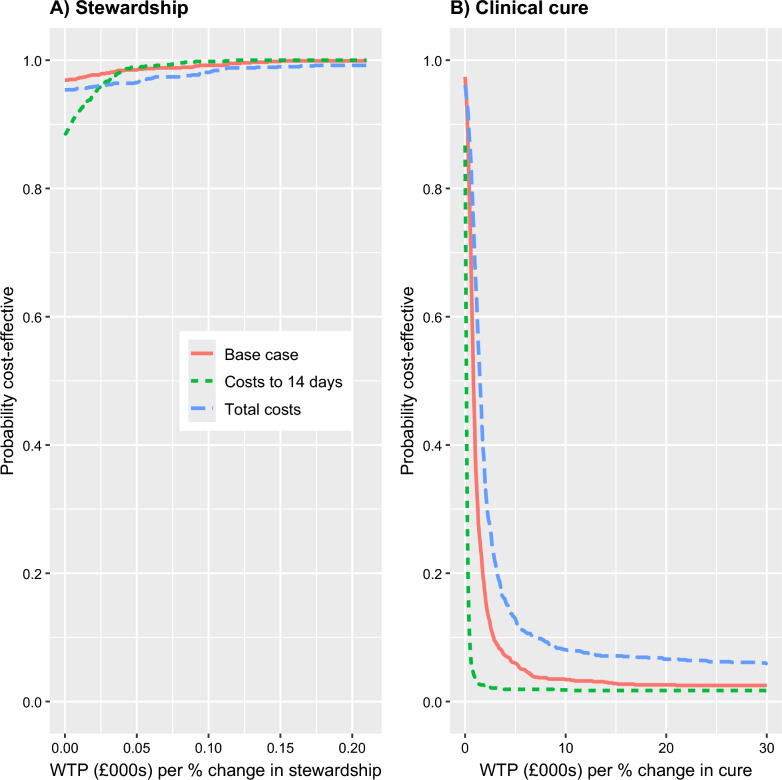
Results: We found lower total ICU costs (including PCR costs) in the intervention (PCR-guided therapy) group. Average costs were £40,951 for standard of care compared with £33,149 for the intervention group, a difference of - £7,802 (95% CI: - £15,696, £92). For antibiotic stewardship, the PCR-guided therapy was both less costly and more effective than routine patient management. For clinical cure, we did not find PCR-guided therapy to be cost-effective due to fewer cases being cured in the intervention group.
Conclusions: We found lower average ICU costs with the Pneumonia Panel. The pneumonia panel was cost-effective in terms of antibiotic stewardship, but not clinical cure.
Trial registration: Registered as ISRCTN16483855 on 5th August 2019.
Keywords: Antibiotic stewardship; Cost-effectiveness; Hospital-acquired pneumonia (HAP); Molecular diagnostics; Point-of-care; Rapid PCR; Syndromic PCR; Ventilator-associated pneumonia (VAP).
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: As noted in the main clinical paper [13] ethics approval was from the London-Brighton and Sussex Research Ethics Committee (19/LO/0400). Consent was deferred: adult patients or their consultees were approached for written consent or assent as soon as possible after randomisation. When incapacitated patients regained capacity they were approached for retrospective consent directly. For children, parents or guardians were approached for consent, and older children were approached for assent. The INHALE WP3 trial was registered as ISRCTN16483855 on 5th August 2019. Consent for publication: Not applicable. Competing interests: VE reports consultancy and speaker fees from bioMérieux, personal fees from Alchemab Therapeutics, and in-kind contributions from Inflammatix Inc. VG reports speaker fees from bioMérieux and consultancy fees from Gilead, MSD, Pfizer and Shionogi. DML reports personal fees from Adjutec, AstraZeneca, bioMérieux, Centauri, GenPax, GSK, Hikma, Merck/MSD, Nordic, Paion, Pfizer, Shionogi, Sumitovant, Summit, Thermofisher, and Zambon. He also reports shareholdings from GenPax, GSK, Merck, and PerkinElmer/Revvity, comprising less than 10% of portfolio value. He also has nominated holdings in Arecor, Celadon Pharmaceuticals, Destiny Pharma, Eluceda Ltd., Genedrive, Poolbeg, Optibiotix, Probiotix Health, SkinBiotherapeutics, Trellus and Verici Dx (all of which have research/products pertinent to medical and diagnostic innovation) through Enterprise Investment Schemes but has no authority to trade these shares directly. All are outside the submitted work. All other authors declare no competing interests.
Figures

References
-
- American Thoracic Society Infectious Diseases Society of America. Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Healthcare-associated Pneumonia. Am J Respir Crit Care Med. 2005;171(4):388–416. - PubMed
-
- NICE: Pneumonia in adults: diagnosis and management: Clinical guideline. In. Manchester; 2014.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Research Materials
