

Bloodstream infections: trends in etiology and antimicrobial resistance in 10 years in Eastern Nepal
- PMID: 40781612
- PMCID: PMC12333069
- DOI: 10.1186/s12879-025-11413-4
Bloodstream infections: trends in etiology and antimicrobial resistance in 10 years in Eastern Nepal
Abstract
Background: Bloodstream infections (BSIs) are defined as the presence of viable infectious microorganisms in the bloodstream causing clinical illness. Early diagnosis and prompt administration of antimicrobial therapy in patients with BSIs have been shown to reduce both mortality and morbidity. Local and regional antimicrobial resistance (AMR) surveillance contributes to national efforts, which in turn support global strategies to combat AMR. Therefore, this study was conducted to determine the profile and antimicrobial susceptibility pattern of organisms associated with of BSIs, with the aim of guiding antimicrobial policy.
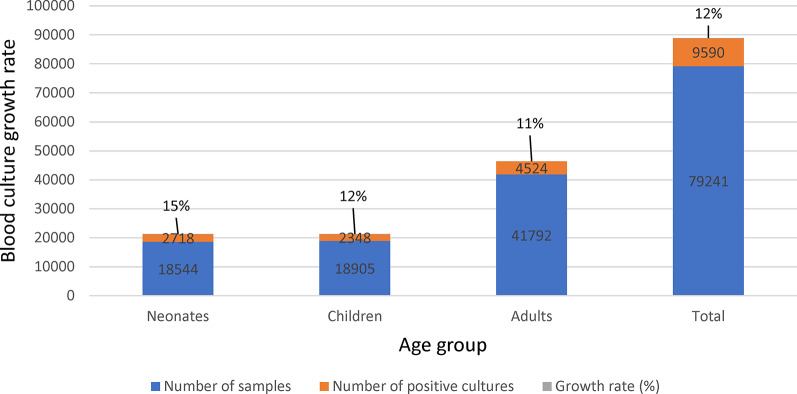
Materials and methods: This was a hospital-based retrospective study. Laboratory records of all blood samples submitted for culture and sensitivity testing to the Department of Microbiology, B. P. Koirala Institute of Health Sciences (BPKIHS) over a 10-year period (January 2012 to December 2021) were analyzed. All the blood samples were processed using conventional culture methods. Bacterial pathogens were identified, and their antimicrobial susceptibility was determined using standard microbiological procedures. Patient's demographic data, organism profiles and antimicrobial susceptibility patterns were analyzed using Microsoft excel.
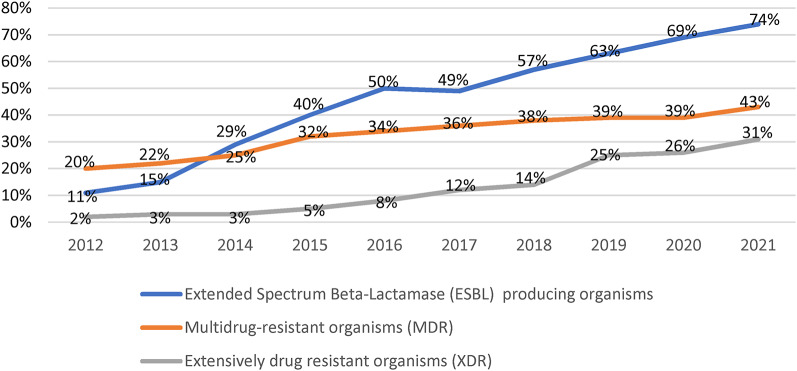
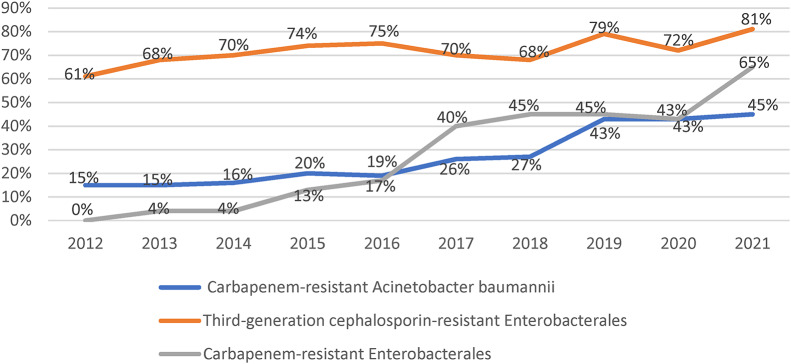
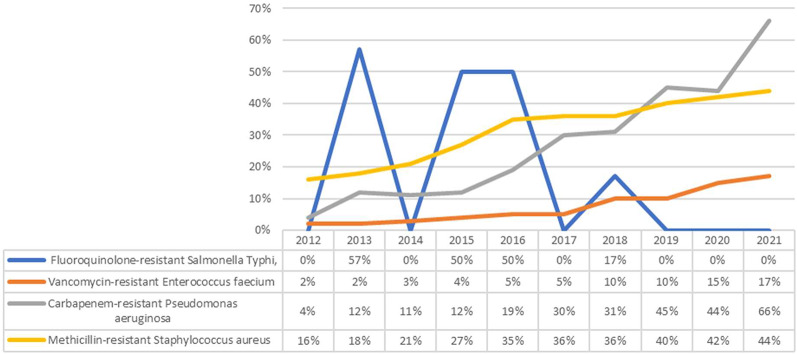
Results: A total of 79,241 samples were received during the study period. Bacterial growth was observed in 9590 samples with culture positivity of 12.1%. Staphylococcus aureus (44%, n = 4,210) was the most common organism, followed by Acinetobacter baumannii (18%, n = 1,762), Pseudomonas aeruginosa (9%, n = 820), Klebsiella pneumoniae (8%, n = 752) and Enterococcus spp (8%, n = 741). All resistant phenotypes increased over the years, extended-spectrum beta-lactamase (ESBL) producers rising from 11 to 74%, multidrug-resistant (MDR) organisms from 20 to 43%, and extensively drug-resistant (XDR) organisms from 2 to 31%. Among WHO critical priority pathogens, there was a significant rise in third-generation cephalosporin-resistant Enterobacterales (61-81%), carbapenem-resistant Enterobacterales (0-65%) and carbapenem-resistant A. baumannii (15-45%). Similarly, high-priority pathogens such as methicillin-resistant Staphylococcus aureus (MRSA) increased from 16 to 44%, vancomycin-resistant Enterococcus faecium (VRE) from 2 to 17%, and carbapenem-resistant Pseudomonas aeruginosa from 4 to 66%.
Conclusion: The rising prevalence of MDR and XDR organisms underscores the growing challenge of managing BSIs effectively, especially in resource-limited settings.
Keywords: Antimicrobial resistance; Bloodstream infection; Eastern Nepal.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This study was performed in line with the principles of the Declaration of Helsinki. Ethical approval was obtained from the institutional review committee (IRC) of B. P Koirala Institute of Health Sciences (BPKIHS) (code number: 1026/017). The need for consent to participate was waived by IRC of BPKIHS. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
References
-
- Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013. 10.1111/1469-0691.12195. - PubMed
-
- Leibovici L, Konisberger H, Pitlik SD, Samra Z, Drucker M. Bacteremia and fungemia of unknown origin in adults. Clin Infect Dis. 1992. 10.1093/clinids/14.2.436. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
