

Cardiometabolic risk stratification in pediatric obesity: evaluating the clinical utility of fasting insulin and BMI-SDS
- PMID: 40781672
- PMCID: PMC12335099
- DOI: 10.1186/s12933-025-02882-7
Cardiometabolic risk stratification in pediatric obesity: evaluating the clinical utility of fasting insulin and BMI-SDS
Abstract
Background: Patients with obesity during childhood have an increased risk of fatal and non-fatal cardiovascular events during adulthood. The severity of obesity is commonly determined by BMI. However, children with relatively low BMI may have high cardiometabolic risk. Indeed, BMI-based obesity classifications might miss children at high cardiometabolic risk. Insulin has been suggested as a marker of cardiometabolic risk. In this study, we therefore estimated and compared cardiometabolic risk using either the BMI standard deviation score (BMI-SDS) or fasting insulin in an international cohort of children and adolescents with obesity and lean controls.
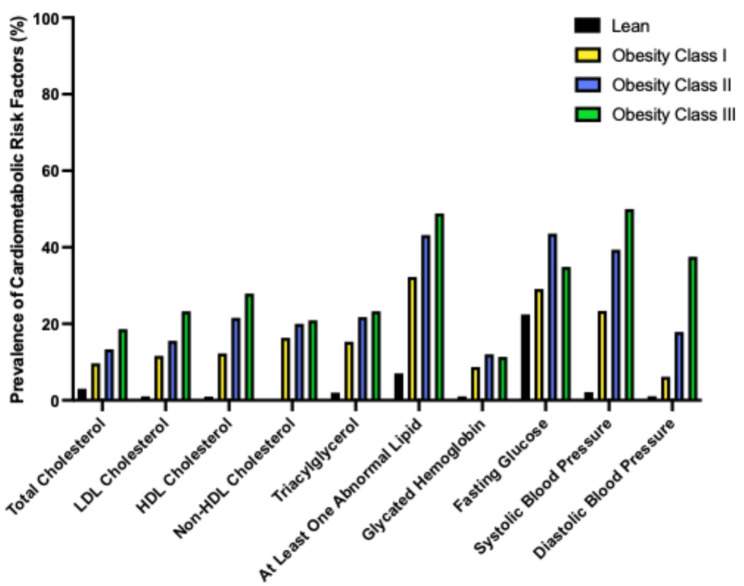
Methods: Study participants (712 with obesity and 99 lean controls), aged 3 to 18 years, were categorized according to their BMI-SDS as lean or obesity class I, II, or III, or by their fasting insulin quartiles as quartile 1, 2, 3, or 4 with the lean subjects in a separate control group. Prevalence of cardiometabolic risk factors was assessed in each group. Sensitivity and specificity analyses for cardiometabolic risk were conducted for both BMI-SDS and fasting insulin. Multiple regression, logistic regression, and receiver operating characteristic (ROC) analyses were performed between fasting insulin, BMI-SDS and cardiometabolic risk factors.
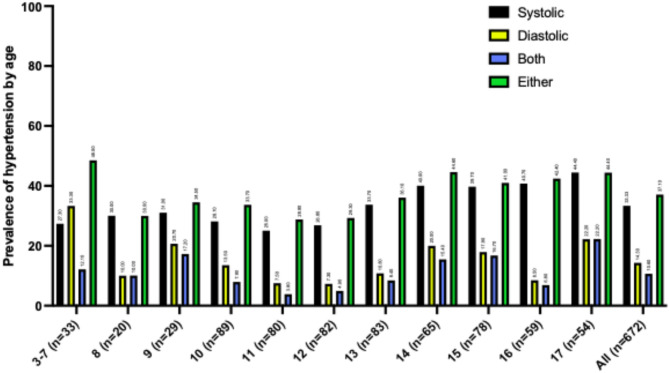
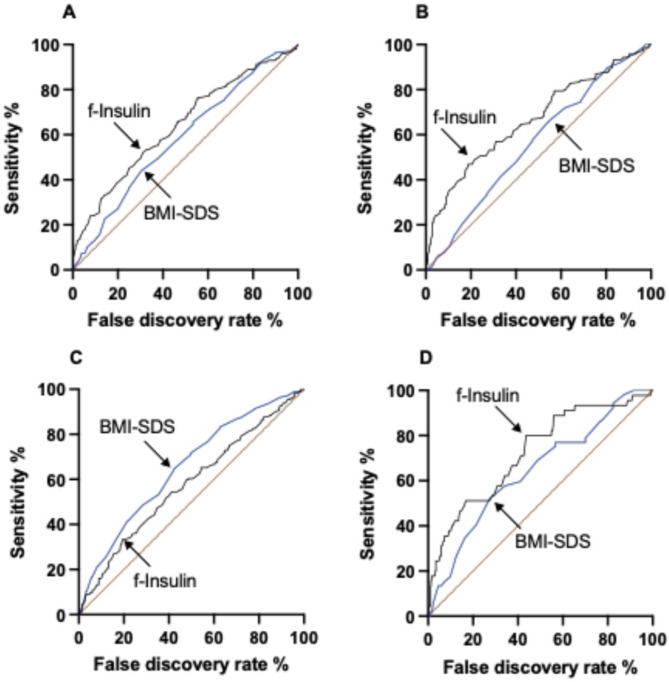
Results: An elevated prevalence of the cardiometabolic risk factors dyslipidemia, dysglycemia and hypertension was observed in both increasing BMI-SDS classes and increasing fasting insulin quartiles. Fasting insulin demonstrated higher areas under the curve (AUC) for detecting dyslipidemia, dysglycemia, and the combination of dyslipidemia, dysglycemia, and hypertension, compared to BMI-SDS. BMI-SDS demonstrated a higher AUC for detecting hypertension compared to fasting insulin. The same patterns were seen for the logistic regression. However, fasting insulin had an overall stronger association with the cardiometabolic risk factors studied compared to BMI-SDS.
Conclusions: In children and adolescents with obesity, fasting insulin provides complementary information to BMI-SDS in identifying those with elevated cardiometabolic risk factors. While neither marker alone offers strong predictive accuracy, incorporating fasting insulin into clinical assessment may help prioritize individuals who require more detailed evaluation. An elevated fasting insulin value may warrant further investigation among children and adolescents with obesity, independent of obesity class based on BMI-SDS.
Keywords: BMI-SDS; Cardiometabolic risk; Cardiovascular disease; Cardiovascular risk factors; Dysglycemia; Dyslipidemia; Hypertension; Insulin; Obesity; Pediatric obesity.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The study was performed in accordance with the Declaration of Helsinki and approved by both the regional ethics committee in Uppsala (registration numbers 2010/036 and 2012/318) and in Salzburg (registration number EK1544/2012). Written informed consent was obtained from adolescents and their legal guardians 12 years or older, or by the legal guardians in case of age under 12 years. Participation was voluntary, and withdrawal of consent without any reason needed was possible throughout the entirety of the study. Consent for publication: All participants and their legal guardians provided consent for publication. Competing interests: The authors declare no competing interests.
Figures

References
-
- Skinner AC, Perrin EM, Moss LA, Skelton JA. Cardiometabolic risks and severity of obesity in children and young adults. N Engl J Med. 2015;373(14):1307–17. - PubMed
-
- Rodriguez PJ, Do D, Gratzl S, Cartwright BMG, Stucky NL, R DW. Treatment of obesity in US children and adolescents before and after the AAP guidelines [Internet]. medRxiv; 2024 [cited 2024 Nov 20]. p. 2024.10.25.24316147. Available from: https://www.medrxiv.org/content/10.1101/2024.10.25.24316147v1
-
- Deanfield J, Verma S, Scirica BM, Kahn SE, Emerson SS, Ryan D, et al. Semaglutide and cardiovascular outcomes in patients with obesity and prevalent heart failure: a prespecified analysis of the SELECT trial. The Lancet. 2024;404(10454):773–86. - PubMed
-
- Kosiborod MN, Abildstrøm SZ, Borlaug BA, Butler J, Rasmussen S, Davies M, et al. Semaglutide in patients with heart failure with preserved ejection fraction and obesity. N Engl J Med. 2023;389(12):1069–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 279153/Seventh Framework Programme
- 2020-02417/Sweden's Innovation Agency Vinnova
- 2020-02417/Sweden's Innovation Agency Vinnova
- 2020-02417/Sweden's Innovation Agency Vinnova
- 2020-02417/Sweden's Innovation Agency Vinnova
- CMP22-0014/Swedish Foundation for Strategic Research
- CMP22-0014/Swedish Foundation for Strategic Research
- CMP22-0014/Swedish Foundation for Strategic Research
- CMP22-0014/Swedish Foundation for Strategic Research
- DIA2023-781/Swedish Diabetes Association
- DIA 2016-146/Swedish Diabetes Association
- DIA2023-781/Swedish Diabetes Association
- DIA2023-781/Swedish Diabetes Association
- 2016-01040/Swedish Research Council
- 2019-01456/Swedish Research Council
- 2019-01456/Swedish Research Council
- RFR 158161, RFR 233041, RFR 309901/Uppsala-Örebro Regional Research Council
- RFR 158161, RFR 233041, RFR 309901/Uppsala-Örebro Regional Research Council
- RFR 158161, RFR 233041, RFR 309901/Uppsala-Örebro Regional Research Council
- 160504/Family Ernfors Foundation
- 160504/Family Ernfors Foundation
LinkOut - more resources
Full Text Sources
Medical
