

Hybrid phantom for lung CT: Design and validation
- PMID: 40781832
- PMCID: PMC12334903
- DOI: 10.1002/mp.17990
Hybrid phantom for lung CT: Design and validation
Abstract
Background: CT lung imaging protocols need to be optimized. This claim is especially important due to the possible introduction of low-dose CT (LDCT) for lung cancer screening. Given the incorporation of non-linear reconstructions and post-processing, the use of phantoms that consider task-based evaluation is needed. This is also true for acceptance and continuous QC use.
Purpose: To present and validate a lung-CT hybrid phantom composed of two setups, one for task-based image quality metrics and the other anthropomorphic.
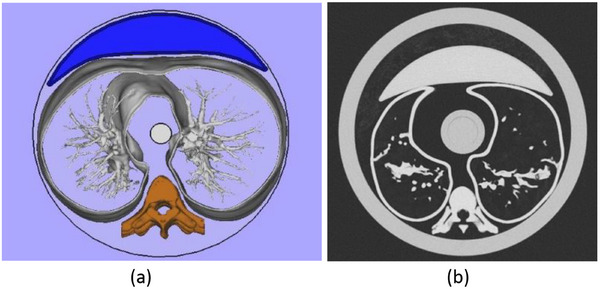
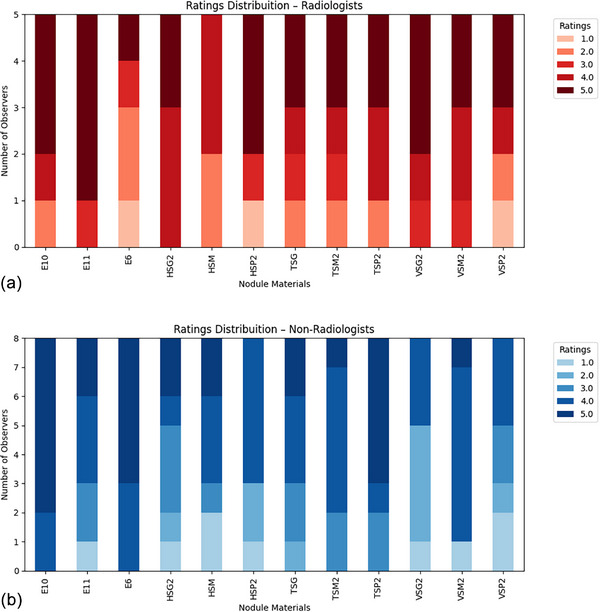
Methods: The task-based metrics setup was based on the well-known Mercury phantom and the anthropomorphic setup named Freddie (from Figure of Merit Performance evaluation of Detectability in Diagnostic CT Imaging Equipment) was designed with the same basic dimensions of the Mercury phantom, but including pieces and materials for mimicking chest structures, such as tracheobronchial tree and lung parenchyma. This setup allows the inclusion of pieces of different sizes to mimic ground-glass opacities, and sub-solid and solid lung nodules. The validation of the phantom adopted three methods: comparative evaluation of the attenuation properties and the corresponding Hounsfield Units (HU) values of the selected materials; image assessment according to five chest radiologists and eight non-radiologists' observations (reader study), and measurement of task-based metrics. Images of both setups were acquired using two clinical thorax protocols, both using automatic tube current modulation (TCM). Two x-ray filter combinations were adopted. The images were reconstructed using a deep learning-based algorithm.
Results: The agreement of nominal and observed HU values in the task-based setup was within 15%, except for three (TangoBlack+, VeroClear, and HIPS) of the materials employed in the phantom construction, at some beam energies. In the reader study, synthetic solid nodules printed in VeroClear received average Likert scores 4.0 (range 3.0-4.0) from radiologists and 3 (range 2.6-3.8) from non-radiologists, printed in TangoBlack+ received an average Likert score of 3.9 (range 3.8-4.2) from radiologists and 4.0 (range 3.8-4.4) from non-radiologists, while those printed in HIPS scored an average Likert of 3.8 (range 3.3-3.9) from radiologists and 3.3 (range 3.1-3.3) from non-radiologists. The synthetic ground-glass opacities (GGO) nodules manufactured in EVA received an average Likert score of 3.8 (range 2.8-4.6) from radiologists and 4.3 (range 3.6-4.8) from non-radiologists. The task-based setup demonstrated detectability index variations across protocols influenced by the dose levels, voltage, and x-ray beam filtration used.
Conclusions: The novelty of the proposed design is concentrated on the possibility of associating the response of the task-based setup (Mercury) with a patient-based setup (Freddie) in a unique phantom. This hybrid design enhances the potential to apply the detectability index for optimizing CT protocols in clinical scenarios.
Keywords: 3D printing; LDCT; anthropomorphic phantom; lung imaging.
© 2025 The Author(s). Medical Physics published by Wiley Periodicals LLC on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures










References
-
- De Koning HJ, van der Aalst CM, De Jong PA, et al. Reduced lung‐cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382(6):503‐513. - PubMed
-
- Carey S, Kandel S, Farrell C, et al. Comparison of conventional chest x ray with a novel projection technique for ultra‐low dose CT. Med Phys. 2021;48(6):2809‐2815. - PubMed
-
- Lee HY. Time to scrutinize and revise the fine print of lung cancer screening using low‐dose CT: seeking greater confidence in cancer detectability. Radiology. 2022;303(1):213‐214. - PubMed
Publication types
MeSH terms
Grants and funding
- 2018/05982-0/Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP)
- 2022/11457-0/Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP)
- 2023/03945-8/Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP)
- 2021/14688-0/Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP)
- 141335/2021-1/Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq)
- 131691/2021-0/Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq)
- 138533/2022-9/Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq)
- 302986/2023-5/Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq)
- 311657/2021-4/Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq)
LinkOut - more resources
Full Text Sources
Medical
