

Effect of intrapartum azithromycin on early childhood gut mycobiota development: post hoc analysis of a double-blind randomized trial
- PMID: 40783383
- PMCID: PMC12335549
- DOI: 10.1038/s41467-025-62142-w
Effect of intrapartum azithromycin on early childhood gut mycobiota development: post hoc analysis of a double-blind randomized trial
Abstract
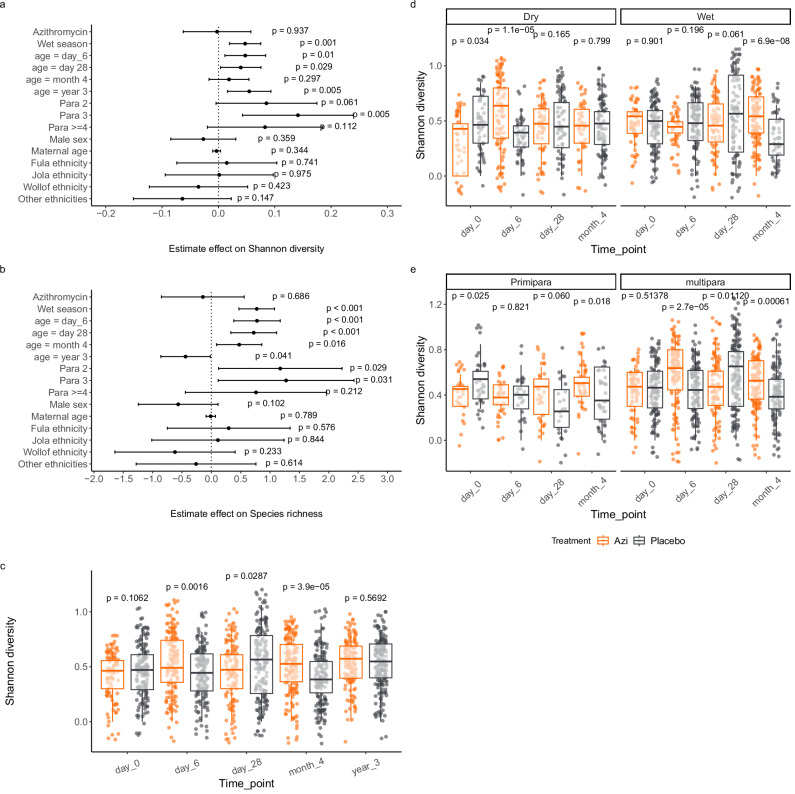
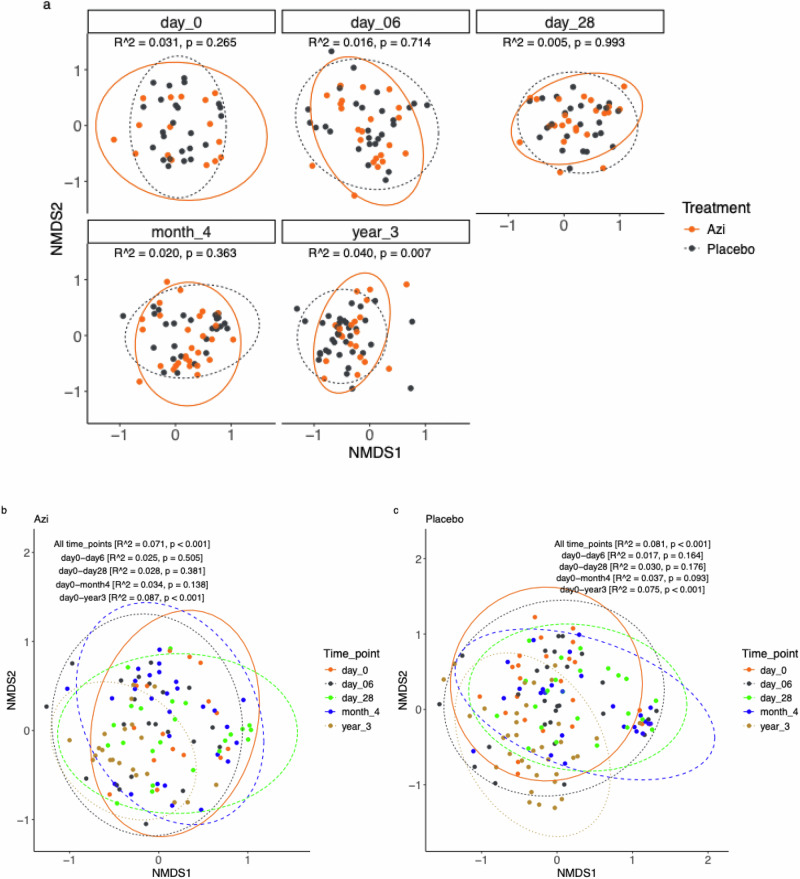
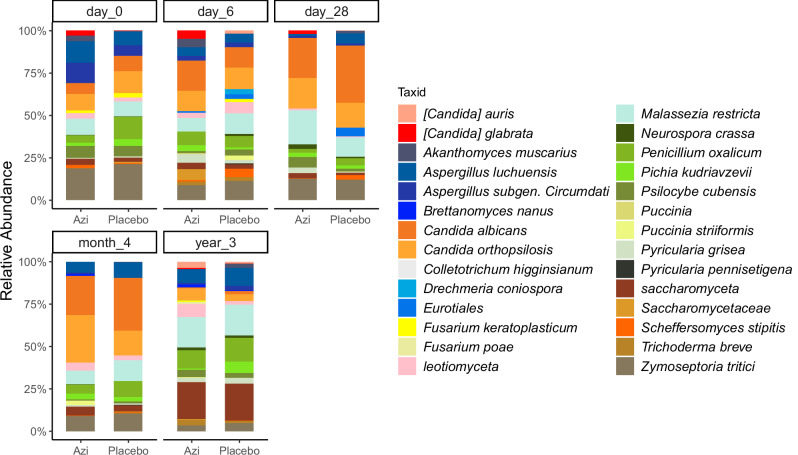
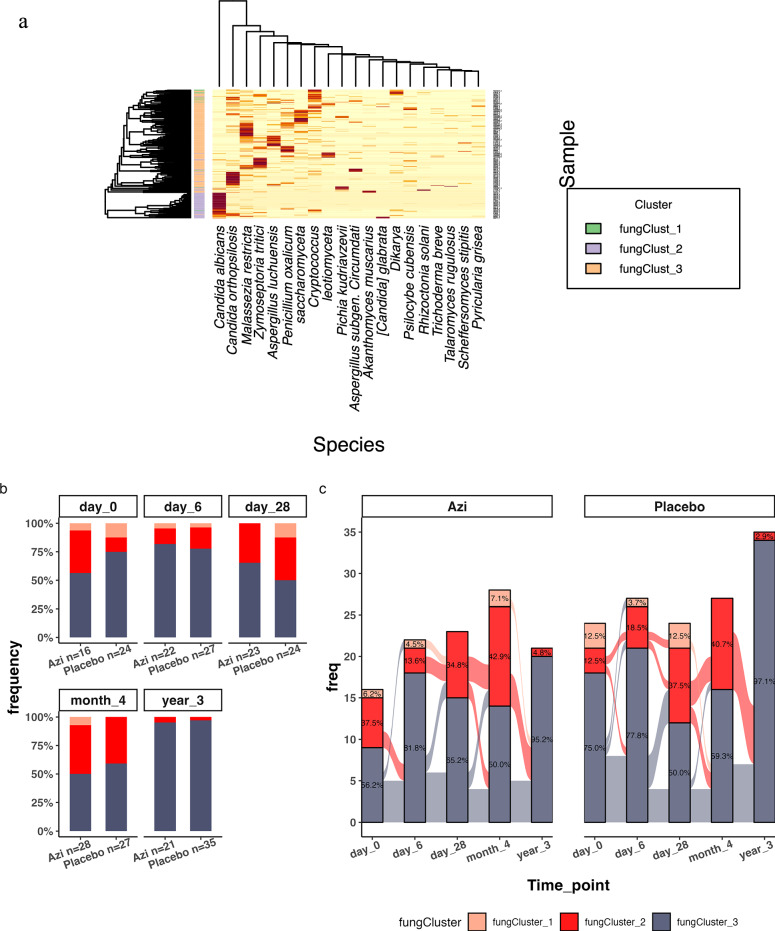
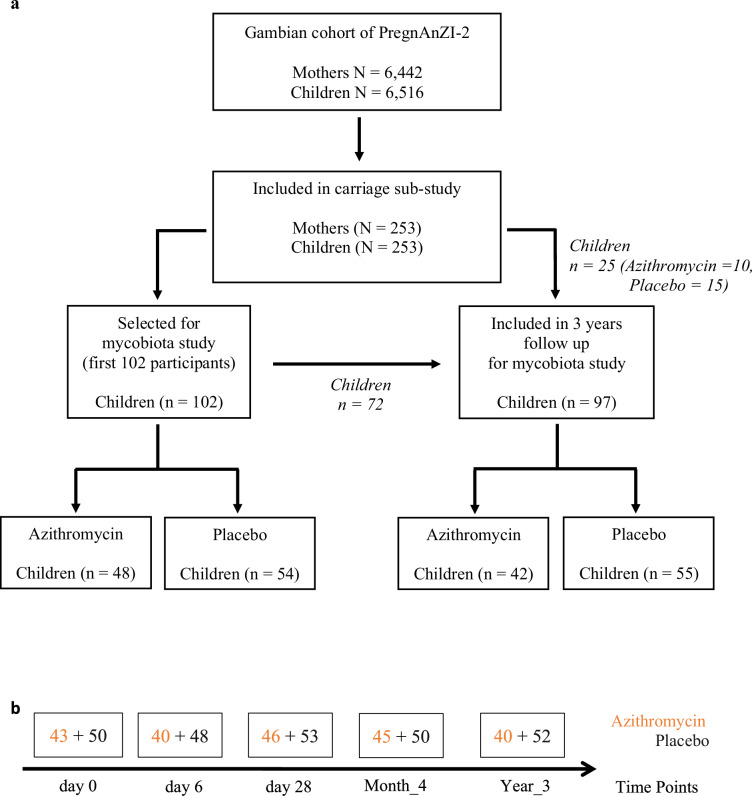
Intrapartum azithromycin prophylaxis reduced maternal infections but showed no effect on neonatal sepsis and mortality. Although antibiotic exposure may indirectly alter the mycobiota (community of fungi that live in a given environment), there is no data available on how intrapartum azithromycin impacts gut mycobiota development. We hereby assess the impact of intrapartum azithromycin on gut mycobiota development from birth to the age of three years, by ITS2 gene profiling of rectal samples from 102 healthy Gambian infants selected from a double-blind randomized placebo-controlled clinical trial (PregnAnZI-2 - ClinicalTrials.org NCT03199547). In the trial, women received 2 g oral azithromycin or placebo (1:1) during labour with the intension of assessing effect on neonatal sepsis or mortality. Secondary objectives included effects on bacterial carriage and resistance, puerperal infections, and infant growth. Our analysis show that season and parity were key factors that influenced gut mycobiota development. Intrapartum azithromycin increased the abundance of Candida orthopsilosis but only in the wet season and did not show different effects by sex of the child. These data suggest that season and parity can be key factors influencing gut mycobiota development and may inform strategies for a wider implementation of intrapartum azithromycin intervention.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
References
-
- WHO. Maternal mortality. https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (2024).
-
- Africa’s advances in maternal, infant mortality face setbacks: WHO report. WHO, Regional Office for Africa. https://www.afro.who.int/news/africas-advances-maternal-infant-mortality... (2022).
-
- WHO. Newborn mortality. https://www.who.int/news-room/fact-sheets/detail/newborn-mortality (2024).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
