

Clinical analysis of histiocytic necrotizing lymphadenitis in adults with fever of unknown origin: a retrospective study
- PMID: 40783524
- PMCID: PMC12335763
- DOI: 10.1186/s13000-025-01695-2
Clinical analysis of histiocytic necrotizing lymphadenitis in adults with fever of unknown origin: a retrospective study
Abstract
Purpose: To comprehensively analyze the clinical data of histiocytic necrotizing lymphadenitis (HNL) in adults with fever of unknown origin (FUO), with the aim of enabling precise diagnosis.
Patients and methods: A total of 15 HNL patients with FUO were enrolled. The analysis encompassed clinical manifestations, laboratory parameters 18F-Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography (18F-FDG PET/CT) imaging profiles, pathological features and therapeutic responses.
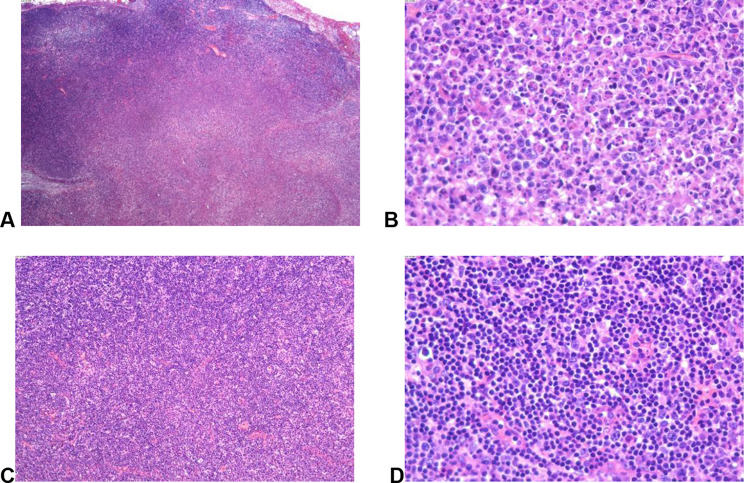
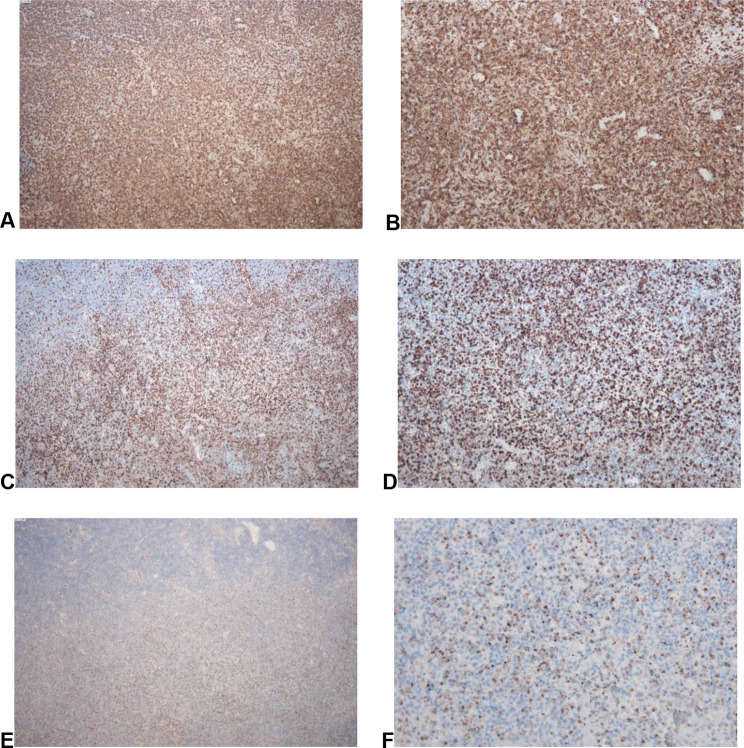
Results: All patients presented with fever and lymphadenopathy (predominantly cervical). Laboratory findings included leukopenia (3.28 × 10⁹/L [2.40-4.97]), elevated LDH (306 U/L [187-524]), ESR (40 mm/h [30-51]), ferritin (457.1 ng/mL [206-1823.3]), and CRP (25 mg/L [6.1-34.8]) 18F-FDG PET/CT detected metabolic lymph node abnormalities in 13 cases, primarily cervical and axillary. The pathological features were extensive coagulative necrosis of lymph nodes with reactive hyperplasia of histiocytes as well as positive or scattered positivity IHC CD3, CD4, CD8 and CD68. Corticosteroid achieved favorable responses, with only 2 cases progressing during follow-up.
Conclusion: In clinical practice, patients with fever and lymphadenopathy should be given due attention. Pathological examination remains the gold standard for diagnosing HNL. Glucocorticoid therapy has proven effective, and the majority of patients with HNL exhibit a favorable prognosis.
Keywords: 18F-FDG PET/CT; Clinical manifestations; Fever of unknown origin; Histiocytic necrotizing lymphadenitis; Pathological features.
© 2025. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: This research adhered to the Declaration of Helsinki principles and was approved by the Ethics Committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology (TJ-IRB20230425). Given its retrospective design, the committee waived informed consent.The study involved no personal identifying info, posed minimal risk to subjects, and couldn’t proceed with consent requirements. The researcher replaced personal info with anonymous identifiers to ensure confidentiality and used aggregate data for publication and presentation to protect subjects’ privacy. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Analysis of the clinical manifestations and 18F-FDG PET-CT findings in 40 patients with histiocytic necrotizing lymphadenitis.Medicine (Baltimore). 2021 Sep 3;100(35):e27189. doi: 10.1097/MD.0000000000027189. Medicine (Baltimore). 2021. PMID: 34477179 Free PMC article.
-
Differential diagnosis of lymphoma with 18F-FDG PET/CT in patients with fever of unknown origin accompanied by lymphadenopathy.J Cancer Res Clin Oncol. 2023 Aug;149(10):7187-7196. doi: 10.1007/s00432-023-04665-7. Epub 2023 Mar 8. J Cancer Res Clin Oncol. 2023. PMID: 36884116 Free PMC article.
-
[Clinical characteristics and treatment in adults and children with histiocytic necroti-zing lymphadenitis].Beijing Da Xue Xue Bao Yi Xue Ban. 2024 Jun 18;56(3):533-540. doi: 10.19723/j.issn.1671-167X.2024.03.022. Beijing Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 38864141 Free PMC article. Chinese.
-
Association of 18F-FDG PET or PET/CT results with spontaneous remission in classic fever of unknown origin: A systematic review and meta-analysis.Medicine (Baltimore). 2018 Oct;97(43):e12909. doi: 10.1097/MD.0000000000012909. Medicine (Baltimore). 2018. PMID: 30412093 Free PMC article.
-
Fluorine-18-fluorodeoxyglucose (FDG) positron emission tomography (PET) computed tomography (CT) for the detection of bone, lung, and lymph node metastases in rhabdomyosarcoma.Cochrane Database Syst Rev. 2021 Nov 9;11(11):CD012325. doi: 10.1002/14651858.CD012325.pub2. Cochrane Database Syst Rev. 2021. PMID: 34753195 Free PMC article.
References
-
- Deaver D, Horna P, Cualing H, Sokol L. Pathogenesis, diagnosis, and management of Kikuchi-Fujimoto disease. Cancer Control. 2014;21:313–21. - PubMed
-
- Patel J, Haltom M, Jackson C. The great masquerader: Kikuchi-Fujimoto disease presenting as fever of unknown origin. J Natl Med Assoc. 2022;113:680–2. - PubMed
-
- Kim CH, Hyun OJ, Yoo IR, Kim SH, Sohn HS, Chung SK. Kikuchi disease mimicking malignant lymphoma on FDG PET/CT. Clin Nucl Med. 2007;32:711–2. - PubMed
-
- Zhang MJ, Xiao L, Zhu YH, Jiang J-j, Jiang M-s, He W. Lymph node uptake of 18F-fluorodeoxyglucose detected with positron emission tomography/computed tomography mimicking malignant lymphoma in a patient with Kikuchi disease. Clin Lymphoma Myeloma Leuk. 2010;10:477–9. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
