

Microbiome-mediated colonization resistance to carbapenem-resistant Klebsiella pneumoniae in ICU patients
- PMID: 40783567
- PMCID: PMC12335454
- DOI: 10.1038/s41522-025-00791-x
Microbiome-mediated colonization resistance to carbapenem-resistant Klebsiella pneumoniae in ICU patients
Abstract
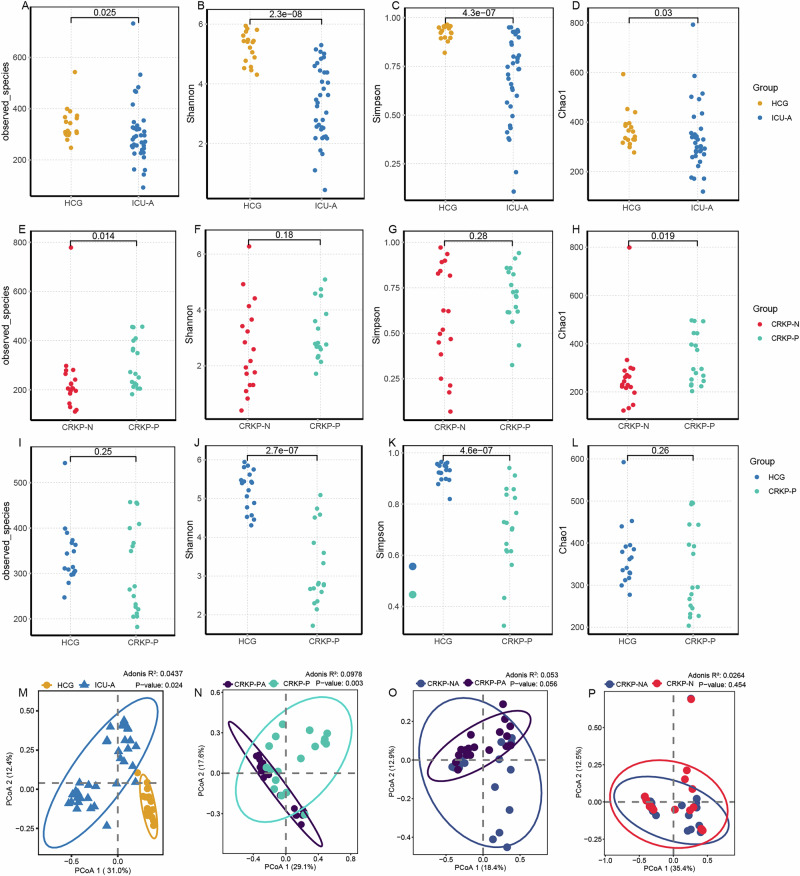
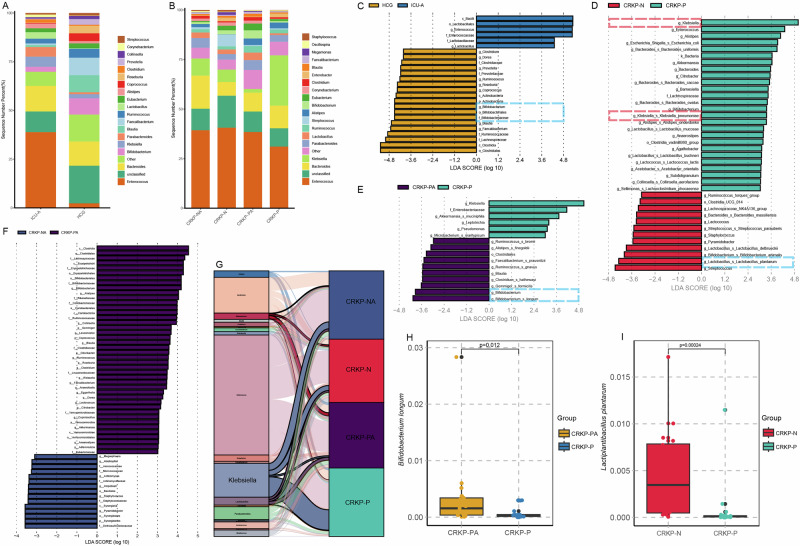
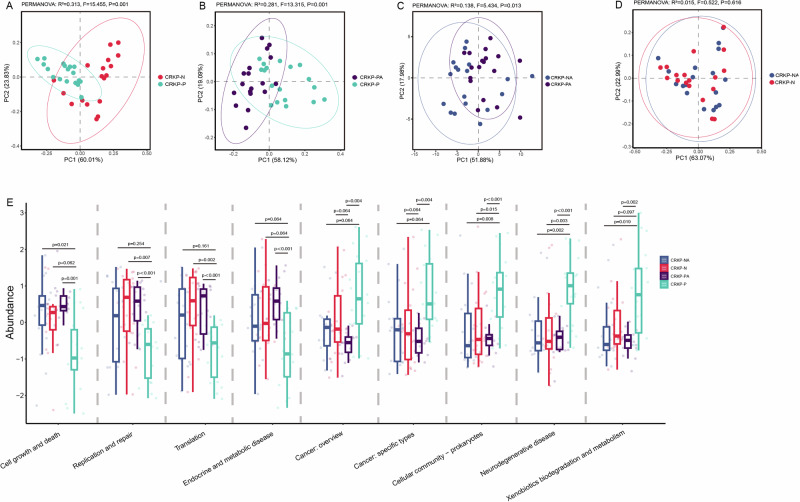
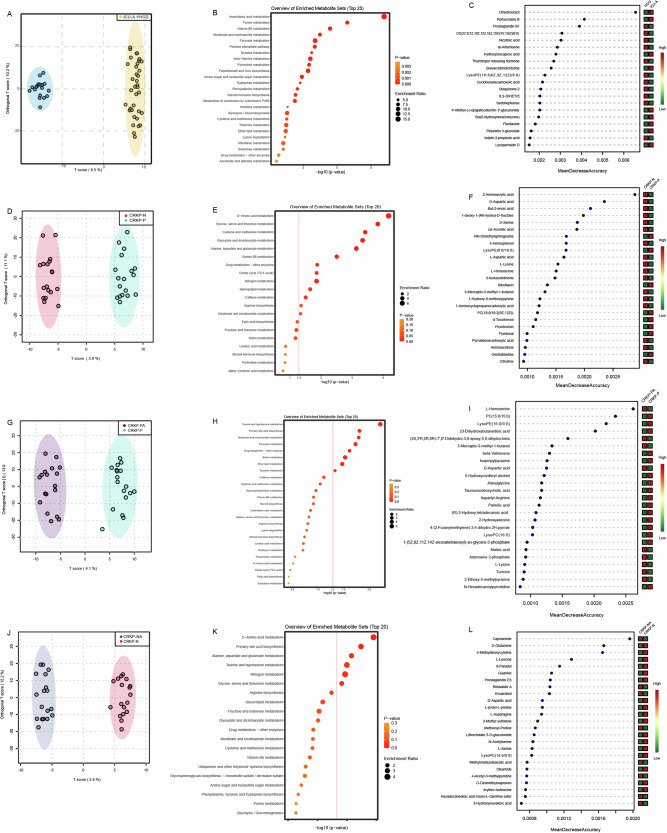
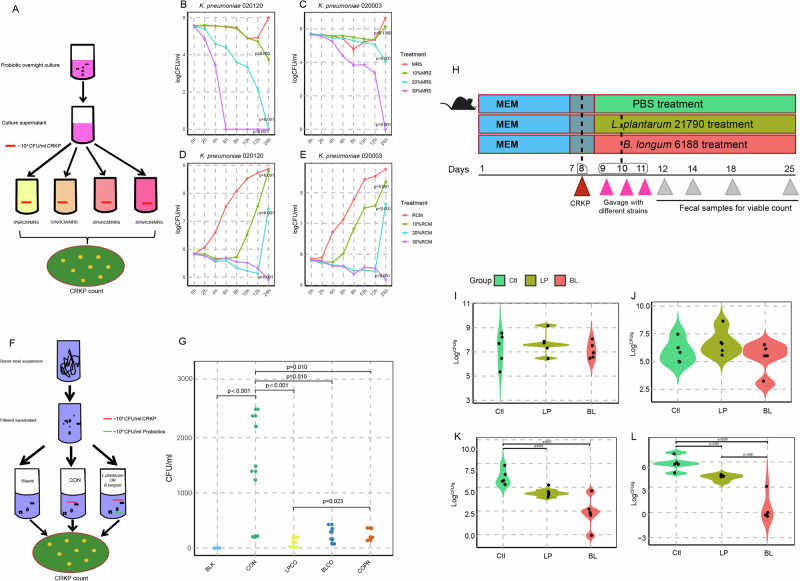
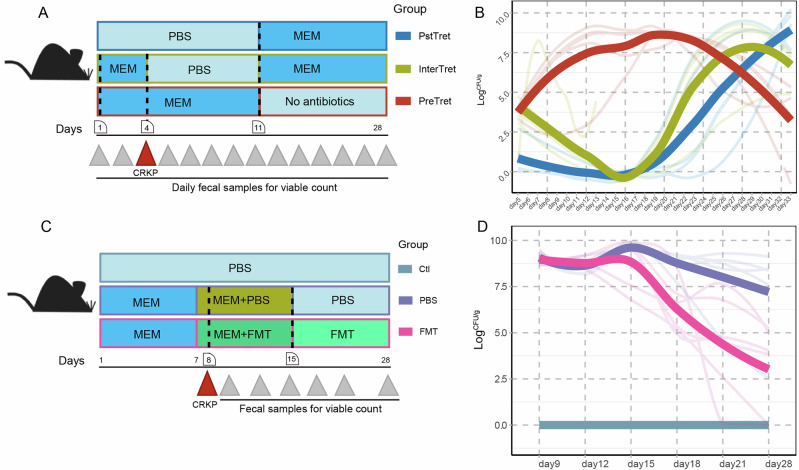
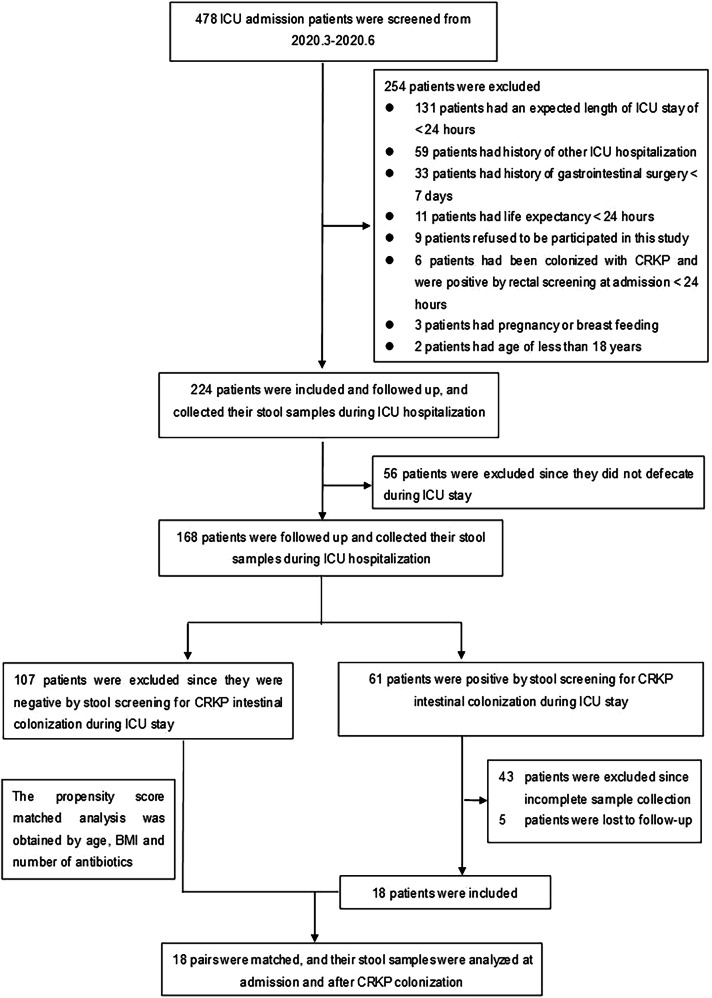
Carbapenem-resistant Klebsiella pneumoniae (CRKP) causes serious intensive care unit (ICU)-acquired infections, yet the mechanisms of microbiota-mediated colonization resistance remain unclear. We analyzed the gut microbiome and metabolic profiles of healthy individuals and ICU patients, distinguishing those with and without CRKP colonization. ICU patients showed distinct microbial communities compared to healthy controls, and CRKP-positive patients exhibited unique microbial and metabolic signatures. We demonstrated that a healthy gut microbiome is essential for providing resistance against CRKP colonization in antibiotic-perturbed mouse with fecal microbiota transplantation (FMT). Both in vitro and in vivo experiments revealed that Lactiplantibacillus plantarum and Bifidobacterium longum as significant contributors to the decolonization of CRKP. Furthermore, we showed that probiotic supplementation or FMT significantly improved CRKP colonization resistance. The findings highlight that a specific gut microbiome is essential for resisting CRKP colonization, and that targeted microbiome restoration may serve as a viable strategy to prevent CRKP colonization in ICU patients.
© 2025. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
Similar articles
-
Carbapenem-resistant Klebsiella pneumoniae gut colonization and subsequent infection in pediatric intensive care units in shanghai, China.Ann Clin Microbiol Antimicrob. 2025 Jul 3;24(1):39. doi: 10.1186/s12941-025-00808-5. Ann Clin Microbiol Antimicrob. 2025. PMID: 40611292 Free PMC article.
-
Study on the correlation between carbapenem-resistant Klebsiella pneumoniae infection strains and intestinal colonization strains in intensive care unit of a tertiary hospital in China.J Glob Antimicrob Resist. 2025 Jun;43:327-336. doi: 10.1016/j.jgar.2025.05.004. Epub 2025 May 19. J Glob Antimicrob Resist. 2025. PMID: 40398678
-
Molecular epidemiology and clinical characteristics of carbapenem-resistant Klebsiella pneumoniae bloodstream and pneumonia isolates.Microbiol Spectr. 2025 Aug 5;13(8):e0063125. doi: 10.1128/spectrum.00631-25. Epub 2025 Jul 9. Microbiol Spectr. 2025. PMID: 40631745 Free PMC article.
-
Incidence and risk factors for subsequent infections among rectal carriers with carbapenem-resistant Klebsiella pneumoniae: a systematic review and meta-analysis.J Hosp Infect. 2024 Mar;145:11-21. doi: 10.1016/j.jhin.2023.12.002. Epub 2023 Dec 12. J Hosp Infect. 2024. PMID: 38092302
-
Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae.Ann Clin Microbiol Antimicrob. 2017 Mar 29;16(1):18. doi: 10.1186/s12941-017-0191-3. Ann Clin Microbiol Antimicrob. 2017. PMID: 28356109 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
