

Impact of prior osteotomy and osteosynthesis on long-term outcomes after total hip arthroplasty : a 1:1 Mahalanobis distance-matched registry study of 5,392 patients
- PMID: 40784669
- PMCID: PMC12335900
- DOI: 10.1302/2633-1462.68.BJO-2025-0067
Impact of prior osteotomy and osteosynthesis on long-term outcomes after total hip arthroplasty : a 1:1 Mahalanobis distance-matched registry study of 5,392 patients
Abstract
Aims: Patients with a history of osteotomy or osteosynthesis pose distinct challenges in total hip arthroplasty (THA) due to altered anatomy and biomechanics. Although THA is an established intervention for degenerative hip disease, limited evidence exists on its long-term outcomes in this cohort, especially regarding revision rates, mortality, and complications. This registry study aimed to determine these outcomes using data from a large national registry.
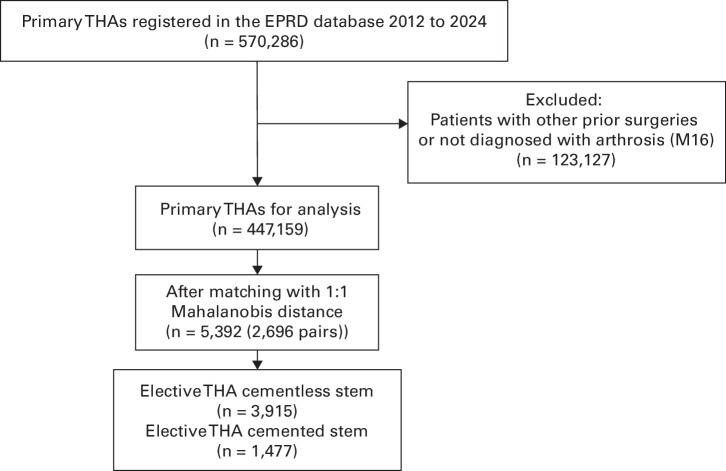
Methods: This registry study analyzed data from the German Arthroplasty Registry (EPRD), which captures approximately 70% of all hip arthroplasties in Germany. Among 418,409 patients undergoing THA between November 2012 and March 2024, 5,392 were included after 1:1 Mahalanobis distance matching for age, sex, BMI, and comorbidities: 2,696 patients with a history of osteotomy or osteosynthesis compared with 2,696 patients without. Kaplan-Meier survival curves estimated revision and mortality risks over an eight-year follow-up.
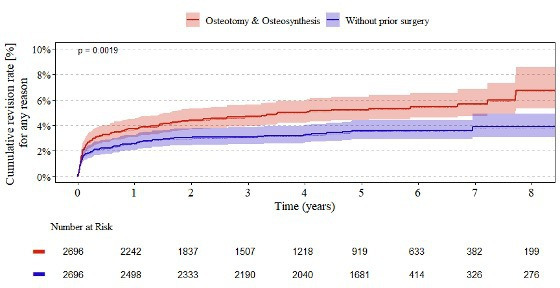
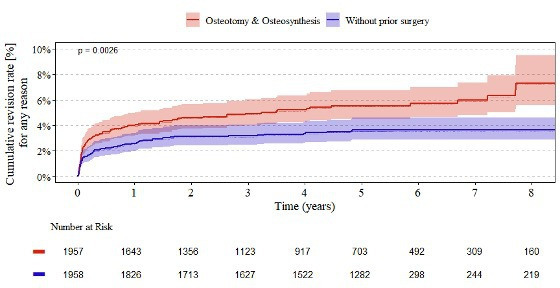
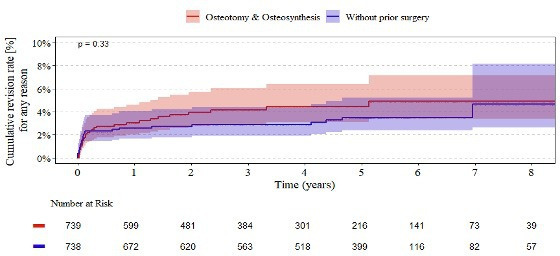
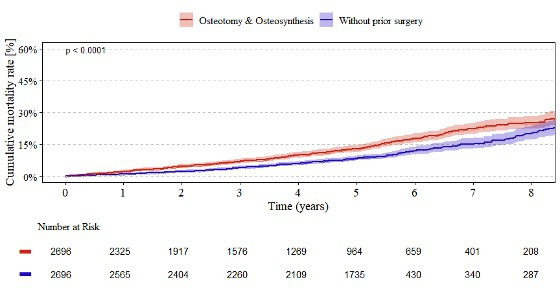
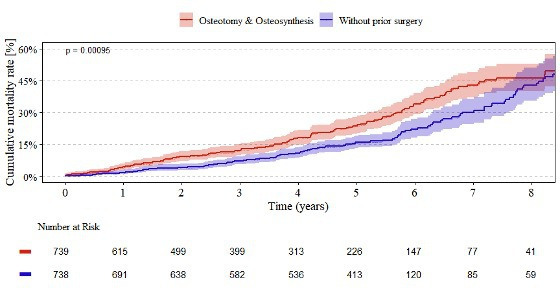
Results: Over eight years, patients with prior osteotomy or osteosynthesis had significantly higher revision (6.8%, n = 183/2,696 vs 3.9%, n = 105/2,696, p = 0.002) and mortality (25.2%, n = 679/2,696 vs 20.4%, n = 550/2,696, p < 0.001) rates than those without prior hip surgery. Infection (17%, n = 22/131 vs 16%, n = 15/94), periprosthetic fracture (14%, n = 18/131 vs 12%, n = 11/94), and dislocation (14%, n = 18/131 vs 8.5%, n=8/94) were leading causes of revision. For cementless femoral components, prior-surgery patients had an eight-year revision rate of 7.3%, n = 143/1,957 compared with 3.6%, n = 71/1,958 (p = 0.003) and a mortality rate of 17.3%, n = 339/1,957 compared with 10.9%, n = 213/1,958 (p < 0.001). For cemented femoral components, revision rates were 4.9%, n = 36/739, compared with 4.7%, n = 35/738 (p = 0.330), and mortality 46.3%, n = 342/739, compared with 43.0%, n = 317/738 (p < 0.001). At one year, the revision rate in the prior-surgery group was already elevated at 3.7% (95% CI 3.1 to 4.5; n = 100/2,696) compared with 2.6% (95% CI 2.0 to 3.3; n = 70/2,696) in controls, diverging further over time.
Conclusion: Patients with prior osteotomy or osteosynthesis undergoing THA face higher long-term revision and mortality risks, particularly with cementless stem fixation. Infection, periprosthetic fracture, and dislocation are key causes of revision.
© 2025 Wagener et al.
Conflict of interest statement
A. Grimberg is a participant in the Implant-Outlier-Workgroup of the German Arthroplasty Registry (EPRD).
Figures

Similar articles
-
Are There Differences in Performance Among Femoral Stem Brands Utilized in Cementless Hemiarthroplasty for Treatment of Geriatric Femoral Neck Fractures?Clin Orthop Relat Res. 2025 Feb 1;483(2):253-264. doi: 10.1097/CORR.0000000000003222. Epub 2024 Aug 15. Clin Orthop Relat Res. 2025. PMID: 39158389
-
Hip arthroplasty for acute femoral neck fracture: Hemiarthroplasty, dual mobility, or conventional total hip arthroplasty? A comparative analysis of 37,169 hip arthroplasties from the Swiss National Joint Registry.Orthop Traumatol Surg Res. 2025 Jul 9:104331. doi: 10.1016/j.otsr.2025.104331. Online ahead of print. Orthop Traumatol Surg Res. 2025. PMID: 40645446
-
No Difference in Revision Rates and High Survival Rates in Large-head Metal-on-metal THA Versus Metal-on-polyethylene THA: Long-term Results of a Randomized Controlled Trial.Clin Orthop Relat Res. 2024 Jul 1;482(7):1173-1182. doi: 10.1097/CORR.0000000000002924. Epub 2023 Dec 12. Clin Orthop Relat Res. 2024. PMID: 38084856 Free PMC article. Clinical Trial.
-
Arthroplasties for hip fracture in adults.Cochrane Database Syst Rev. 2022 Feb 14;2(2):CD013410. doi: 10.1002/14651858.CD013410.pub2. Cochrane Database Syst Rev. 2022. PMID: 35156194 Free PMC article.
-
Surgical interventions for treating intracapsular hip fractures in older adults: a network meta-analysis.Cochrane Database Syst Rev. 2022 Feb 14;2(2):CD013404. doi: 10.1002/14651858.CD013404.pub2. Cochrane Database Syst Rev. 2022. PMID: 35156192 Free PMC article.
References
-
- Parilla FW, Freiman S, Pashos GE, Thapa S, Clohisy JC. Comparison of modern periacetabular osteotomy for hip dysplasia with total hip arthroplasty for hip osteoarthritis-10-year outcomes are comparable in young adult patients. J Hip Preserv Surg. 2022;9(3):178–184. doi: 10.1093/jhps/hnac029. - DOI - PMC - PubMed
-
- Johnsen SP, Sørensen HT, Lucht U, Søballe K, Overgaard S, Pedersen AB. Patient-related predictors of implant failure after primary total hip replacement in the initial, short- and long-terms. A nationwide Danish follow-up study including 36,984 patients. J Bone Joint Surg Br. 2006;88-B(10):1303–1308. doi: 10.1302/0301-620X.88B10.17399. - DOI - PubMed
LinkOut - more resources
Full Text Sources
