

Clinical Benefits of Cartilage Repair in High Tibial Osteotomy Can Only Be Expected in Patients with Successfully Regenerated Cartilage
- PMID: 40785776
- PMCID: PMC12328110
- DOI: 10.4055/cios24409
Clinical Benefits of Cartilage Repair in High Tibial Osteotomy Can Only Be Expected in Patients with Successfully Regenerated Cartilage
Abstract
Background: The clinical benefits of combining cartilage procedures with high tibial osteotomy (HTO) remain undetermined. This study aimed to evaluate the additional clinical benefits by comparing a combined procedure group with an isolated HTO group, with stratification based on the success of cartilage regeneration.
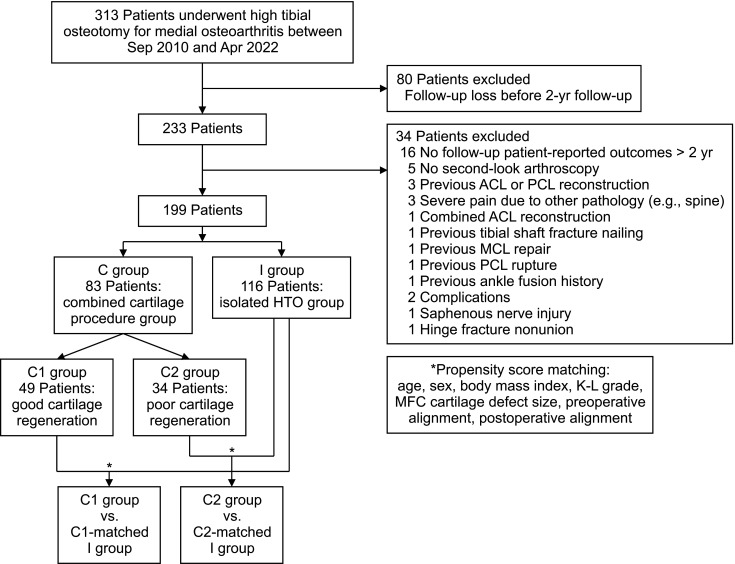
Methods: Patients who underwent medial open-wedge HTO from 2010 to 2022 with a minimum 2-year follow-up were retrospectively reviewed. Patients were divided into 2 groups: HTO + combined cartilage procedures (C group) and isolated HTO (I group). C group was further divided into 2 subgroups based on the medial femoral condyle (MFC) cartilage status assessed on second-look arthroscopy: well-regenerated cartilage (C1 group) and poorly regenerated cartilage (C2 group). Propensity score-matched I groups were formed for each C1 and C2 group (C1-matched and C2-matched group I), based on baseline factors affecting clinical outcomes. Comparative analysis was performed for each matched pair based on patient-reported outcomes (PROs).
Results: A total of 313 patients were retrospectively reviewed in this study, with 199 patients included in the analysis: 83 patients in the C group (49 in the C1 group and 34 in the C2 group) and 116 patients in the I group. Baseline characteristics showed no significant difference between the matched groups after propensity score matching. The mean follow-up period for all groups was approximately 3 years with no significant differences. The C1 group showed significantly better PROs and improved PROs at the final follow-up compared to the C1-matched I group (visual analog scale score, p < 0.001; Lysholm, p = 0.004; Knee injury and Osteoarthritis Outcome Score subscales, p ≤ 0.018). However, the C2 group did not show any differences in PROs compared to the C2-matched I group at the final follow-up.
Conclusions: Only patients with well-regenerated cartilage after combined cartilage repair procedures showed additional clinical outcome improvements with HTO. When considering combined cartilage repair procedures with HTO, selecting appropriate candidates for achieving successful cartilage regeneration is necessary to yield additional clinical benefits.
Keywords: Articular cartilage; Cartilage injuries; Cartilage sugery; Osteoarthritis; Osteotomy.
Copyright © 2025 by The Korean Orthopaedic Association.
Conflict of interest statement
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
Figures




References
-
- Ollivier B, Berger P, Depuydt C, Vandenneucker H. Good long-term survival and patient-reported outcomes after high tibial osteotomy for medial compartment osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2021;29(11):3569–3584. - PubMed
-
- Akizuki S, Shibakawa A, Takizawa T, Yamazaki I, Horiuchi H. The long-term outcome of high tibial osteotomy: a ten-to 20-year follow-up. J Bone Joint Surg Br. 2008;90(5):592–596. - PubMed
-
- Jung SH, Jung M, Chung K, et al. Factors causing unintended sagittal and axial alignment changes in high tibial osteotomy: comparative 3-dimensional analysis of simulation and actual surgery. Am J Sports Med. 2024;52(6):1543–1553. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
