

Evaluation of feasibility and clinical outcomes of robot-assisted pancreaticoduodenectomy after neoadjuvant treatment for patients with advanced pancreatic ductal adenocarcinoma: a retrospective propensity score-matched cohort study
- PMID: 40785812
- PMCID: PMC12329137
- DOI: 10.4174/astr.2025.109.2.61
Evaluation of feasibility and clinical outcomes of robot-assisted pancreaticoduodenectomy after neoadjuvant treatment for patients with advanced pancreatic ductal adenocarcinoma: a retrospective propensity score-matched cohort study
Abstract
Purpose: With neoadjuvant treatment (NAT) broadening the surgical indication for advanced pancreatic cancer, the growing use of robotic platforms in pancreaticoduodenectomy (PD) necessitates the evaluation of its feasibility in advanced pancreatic cancer patients who have undergone NAT.
Methods: We compared clinicopathological outcomes of advanced pancreatic cancer patients who received either robot-assisted or open PD after NAT at a tertiary hospital from 2015 to 2023. Propensity score matching was performed based on age, sex, and TNM staging.
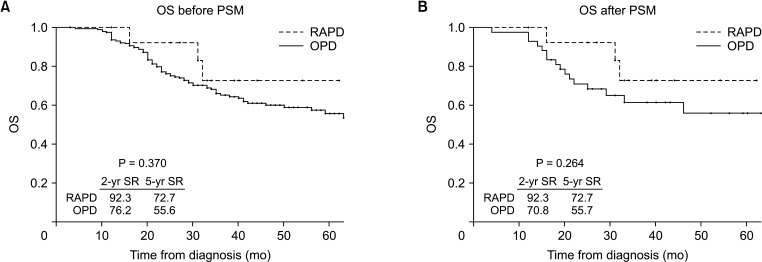
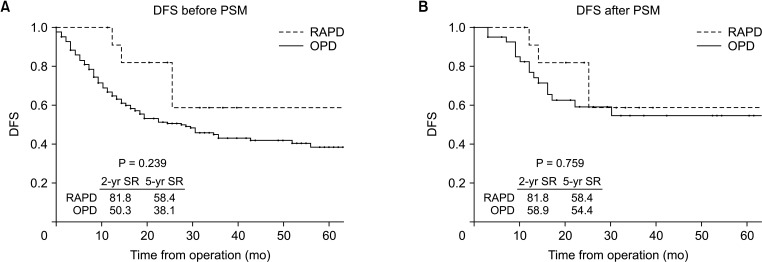
Results: Among 223 patients who received conversion surgery after NAT, 42 open PD and 14 robot-assisted PD patients were matched in a 3:1 ratio. There was a trend of shorter hospital stays (11.4 days vs. 9.8 days, P = 0.218) and less severe postoperative complications (21.4% vs. 7.1%; P = 0.227) in the robot-assisted PD group. Lymph node (LN) yield, LN metastasis rate, and R0 resection rates were similar between the 2 groups. The overall (OS) and disease-free survival (DFS) rates between the 2 groups were comparable (5-year OS rate: 55.7% vs. 72.7%, P = 0.264; 5-year DFS rate: 54.4% vs. 58.4%, P = 0.759).
Conclusion: Robot-assisted PD offers comparable short-term and long-term outcomes to open PD, even in patients undergoing conversion surgery after NAT.
Keywords: Neoadjuvant therapy; Outcomes; Pancreatic neoplasms; Pancreaticoduodenectomy; Robotic surgical procedures.
Copyright © 2025, the Korean Surgical Society.
Conflict of interest statement
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Long-term oncologic outcomes of robot-assisted pancreaticoduodenectomy versus open pancreaticoduodenectomy for pancreatic cancer.Surg Endosc. 2025 Aug;39(8):5097-5106. doi: 10.1007/s00464-025-11833-y. Epub 2025 Jul 9. Surg Endosc. 2025. PMID: 40634729 Free PMC article.
-
Survival Outcomes in Nonmetastatic pT4 Pancreatic Ductal Adenocarcinoma: A SEER Database Analysis Comparing Neoadjuvant Therapy and Upfront Surgery with Propensity Score Matching.Asian Pac J Cancer Prev. 2025 Mar 1;26(3):847-859. doi: 10.31557/APJCP.2025.26.3.847. Asian Pac J Cancer Prev. 2025. PMID: 40156401 Free PMC article.
-
Systematic review and cumulative analysis of oncologic and functional outcomes after robot-assisted radical cystectomy.Eur Urol. 2015 Mar;67(3):402-22. doi: 10.1016/j.eururo.2014.12.008. Epub 2015 Jan 2. Eur Urol. 2015. PMID: 25560797
-
Comparison of laparoscopic versus robot-assisted sugery for rectal cancer after neo-adjuvant therapy: a large volume single center experience.BMC Surg. 2025 Mar 12;25(1):98. doi: 10.1186/s12893-025-02764-5. BMC Surg. 2025. PMID: 40075413 Free PMC article.
-
Open vs robotic-assisted pancreaticoduodenectomy, cost-effectiveness and long-term oncologic outcomes: a systematic review and meta-analysis.J Gastrointest Surg. 2024 Nov;28(11):1933-1942. doi: 10.1016/j.gassur.2024.08.013. Epub 2024 Aug 15. J Gastrointest Surg. 2024. PMID: 39153714
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72:7–33. - PubMed
-
- Jang JY, Han Y, Lee H, Kim SW, Kwon W, Lee KH, et al. Oncological benefits of neoadjuvant chemoradiation with gemcitabine versus upfront surgery in patients with borderline resectable pancreatic cancer: a prospective, randomized, open-label, multicenter phase 2/3 trial. Ann Surg. 2018;268:215–222. - PubMed
-
- Versteijne E, van Dam JL, Suker M, Janssen QP, Groothuis K, Akkermans-Vogelaar JM, et al. Neoadjuvant chemoradiotherapy versus upfront surgery for resectable and borderline resectable pancreatic cancer: long-term results of the Dutch randomized PREOPANC trial. J Clin Oncol. 2022;40:1220–1230. - PubMed
LinkOut - more resources
Full Text Sources
