

Fetal umbilical-portal-systemic venous shunt diagnosed by prenatal ultrasonography and its association with chromosomal abnormalities
- PMID: 40785864
- PMCID: PMC12332682
- DOI: 10.21037/qims-2025-486
Fetal umbilical-portal-systemic venous shunt diagnosed by prenatal ultrasonography and its association with chromosomal abnormalities
Abstract
Background: Fetuses with umbilical-portal-systemic venous shunt (UPSVS) have poor prognosis, and standard prenatal ultrasound planes do not contain the umbilical-portal-systemic venous system. Moreover, UPSVS-related research is limited, and the rate of chromosomal abnormalities remains unknown. It is necessary to further clarify the ultrasound characteristics and prognosis of these fetuses and develop effective diagnostic models. Accordingly, the objective of this study was to examine the ultrasound image characteristics of fetuses with different types of UPSVS using two-dimensional ultrasound combined with spatiotemporal correlation imaging technology (STIC) and analyzed the chromosomal abnormality rate and pregnancy outcomes.
Methods: A retrospective analysis was performed on fetuses with UPSVS as diagnosed via prenatal ultrasound at Gansu Provincial Maternity and Child Care Hospital from January 2020 to September 2024. Chromosome or gene testing results of UPSVS fetuses, ultrasound characteristics, and the prognosis of fetuses with different types of UPSVS were evaluated. Moreover, a search for literature published from 2000 to 2024 on fetal UPSVS and chromosomal abnormalities was conducted.
Results: A total of 53 fetuses were included in the study. The mean gestational age diagnosed by prenatal ultrasound was 22.2±5.2 weeks. Of the fetuses, 35 fetuses underwent amniocentesis, among whom 25.7% (9/35) had chromosomal or genetic abnormalities (6 type I, 1 type II, and 2 type IIIA). There were 20 cases of terminated pregnancy (9 cases had chromosomal or genetic abnormalities, and 11 cases had severe structural abnormalities), and 33 live births, resulting in 11 cases (34.4%, 11/32; one case was lost to follow-up, and the outcome after birth remained unknown) with poor prognoses. In addition, studies related to fetal UPSVS and their chromosomal or genetic abnormalities published from 2000 to 2024 were analyzed to determine the implications (or indications) of prenatal invasive diagnostic techniques, we found that although most UPAVS fetuses have a good prognosis, the abnormality rate of amniocentesis is about 23.2% (types I and II are more common) when accompanied by other structural abnormalities.
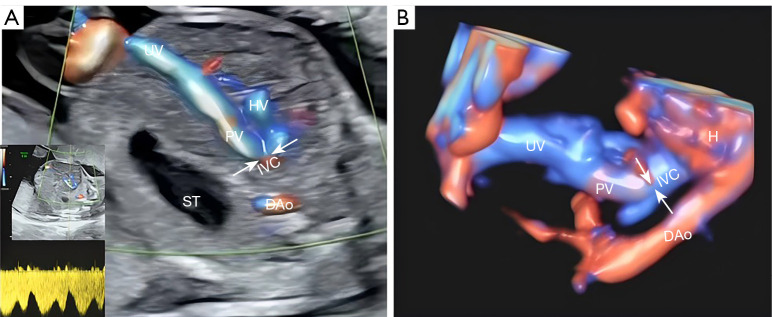
Conclusions: The combination of two-dimensional ultrasound and STIC provides reliable evidence for the diagnosis of UPSVS. Types of UPSVS and chromosomal (or genetic) abnormalities affect the prognosis of UPSVS fetuses.
Keywords: Chromosome abnormality; fetuses; prenatal ultrasound; umbilical-portal-systemic venous shunt (UPSVS).
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-2025-486/coif). The authors have no conflicts of interest to declare.
Figures
References
-
- Wu H, Tao G, Cong X, Li Q, Zhang J, Ma Z, Zhang Z. Prenatal sonographic characteristics and postnatal outcomes of umbilical-portal-systemic venous shunts under the new in-utero classification: A retrospective study. Medicine (Baltimore) 2019;98:e14125 . 10.1097/MD.0000000000014125 - DOI - PMC - PubMed
-
- Lu L, Yao L, Wei H, Hu J, Li D, Yin Y, Su J, Li Q, Zhu S, Tang X, Huang W, Zhu B, Zhang J. Ultrasonographic classification of 26 cases of fetal umbilical-portal-systemic venous shunts and the correlations with fetal chromosomal abnormalities. BMC Pregnancy Childbirth 2023;23:236 . 10.1186/s12884-023-05525-5 - DOI - PMC - PubMed
-
- Jimenez-Gomez J, Güizzo JR, Betancourth Alvarenga J, Santiago Martínez S, Gaspar Perez M, Pina Perez S, Beltrán VP, Loverdos I, Esteva Miró C, Jimenez Arribas P, Sanchez Vazquez B, San Vicente Vela B, Álvarez García N, Nuñez García B. Correlation of Prenatal and Postnatal Diagnosis in Umbilical-Portal-Systemic Venous Shunts. Eur J Pediatr Surg 2023;33:90-5. 10.1055/s-0042-1760379 - DOI - PubMed
LinkOut - more resources
Full Text Sources