

Ultra-low-dose hepatic computed tomography with a novel real-time deep learning-based noise reduction algorithm: a prospective cross-sectional analysis of image quality and lesion detection
- PMID: 40785866
- PMCID: PMC12332563
- DOI: 10.21037/qims-2025-365
Ultra-low-dose hepatic computed tomography with a novel real-time deep learning-based noise reduction algorithm: a prospective cross-sectional analysis of image quality and lesion detection
Abstract
Background: Contrast-enhanced computed tomography (CT) is essential for tumor assessment, but the detection of low-contrast liver lesions remains challenging. Reducing the radiation dose increases image noise, compromising image quality and diagnostic accuracy. Iterative reconstruction (IR) algorithms can reduce noise; however, they can also alter image texture and limit lesion detection. Deep-learning image reconstruction (DLIR) represents a promising alternative, but its efficacy in ultra-low-dose (ULD) hepatic CT for detecting small, low-contrast lesions remains underexplored. Thus, this study aimed to evaluate a novel real-time DLIR algorithm in ULD hepatic CT, focusing on image quality and lesion detection.
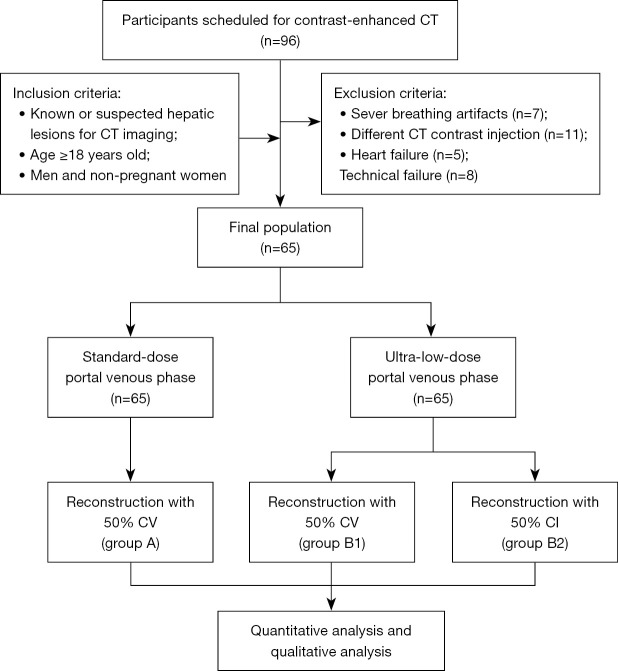
Methods: In total, 65 patients with hepatic lesions underwent both standard-dose and ULD abdominal CT scans during the portal venous phase. The standard-dose protocol (group A) used 120 kV with a signal-to-noise ratio (SNR) of 1.0, and the images were reconstructed using 50% IR. The ULD protocol (group B) used 120 kV with an SNR of 0.5, and the images were reconstructed using 50% IR and 50% DLIR (groups B1 and B2, respectively). The quantitative and qualitative image quality parameters were assessed. The lesion detection rates were evaluated by lesion type and size using the metrics of detection rate, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV).
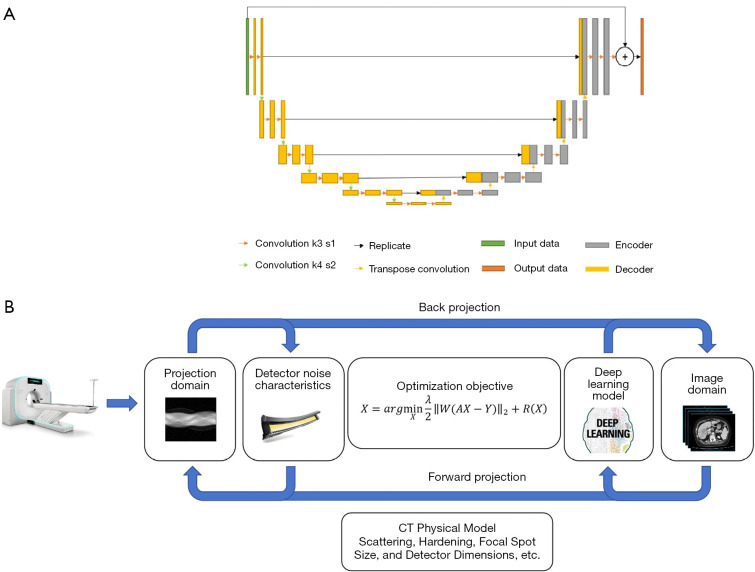
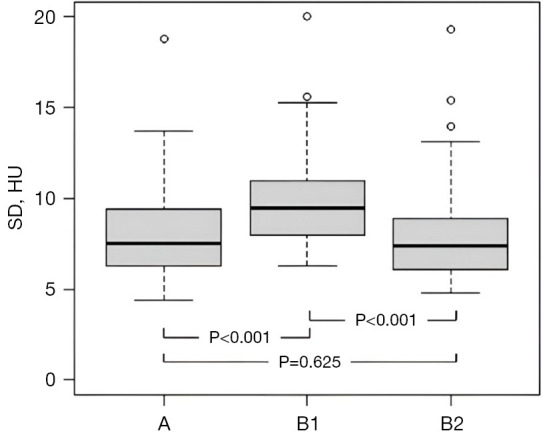
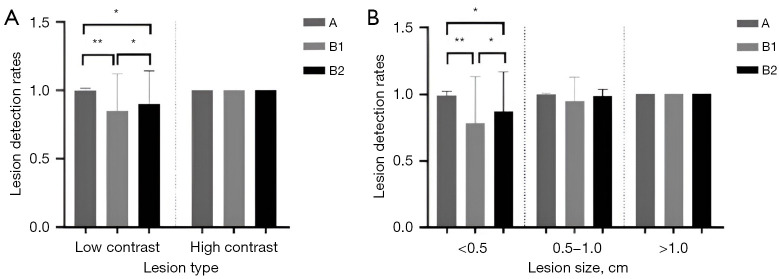
Results: Group B showed a 73.3% reduction in the radiation dose compared to group A (1.5±0.8 vs. 6.9±2.0 mSv, P<0.001). Image noise differed significantly across the protocols: group B1 had the highest noise [10.05±2.94 Hounsfield units (HU)], followed by groups A (8.29±2.82 HU) and B2 (8.04±2.71 HU; all pairwise P<0.05 except group A vs. group B2: P=0.625). The CT values and contrast-to-noise ratios (CNRs) were comparable between groups B2 and A (all P>0.05), while group B2 had a 29.9-42.2% higher CNR than group B1 (all P<0.001). The qualitative assessments confirmed that the image quality and diagnostic acceptability of groups B2 (100%) and A (all P>0.05) were comparable, while the images of group B1 were diagnostically unacceptable (all scores <3). Overall, lesion detection was comparable in groups B2 (90.5%, 133/147) and A (98.0%, 144/147; P>0.05). However, group B2 had a significantly lower detection rate for small lesions (<0.5 cm: 77.8%, 42/54) compared to group A (P<0.05), but outperformed group B1 (57.4%, 31/54; P<0.05). Group B2 also had a significantly improved lesion detection rate and sensitivity for low-contrast lesions (87.2%, 95/109) compared to group B1 (75.2%, 82/109; P<0.05). The novel DLIR algorithm achieved a reconstruction speed of 60 images per second (ips), which was significantly faster than that of other DLIR approaches, while maintaining comparable performance to the IR algorithm.
Conclusions: The combination of tube current reduction with a novel real-time DLIR algorithm enabled ULD abdominal CT to achieve a 73.3% reduction in the radiation dose while maintaining image quality and diagnostic performance for detecting hepatic lesions larger than 0.5 cm.
Keywords: Deep learning; abdomen; computed tomography (CT); radiation dose.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-2025-365/coif). C.X. is an employee of the Neusoft Medical System Company, the manufacturer of the CT system used in this study. The other authors have no conflicts of interest to declare.
Figures

Similar articles
-
Image quality evaluation in deep-learning-based CT noise reduction using virtual imaging trial methods: Contrast-dependent spatial resolution.Med Phys. 2024 Aug;51(8):5399-5413. doi: 10.1002/mp.17029. Epub 2024 Mar 31. Med Phys. 2024. PMID: 38555876 Free PMC article.
-
Comparison of image quality of 40 keV virtual monoenergetic images of vertebral arteries using DLIR and ASIR-V algorithms under a dual-low scanning protocol.Eur J Radiol. 2025 Jul 3;191:112276. doi: 10.1016/j.ejrad.2025.112276. Online ahead of print. Eur J Radiol. 2025. PMID: 40639023
-
Deep Learning Image Reconstruction (DLIR) Algorithm to Maintain High Image Quality and Diagnostic Accuracy in Quadruple-low CT Angiography of Children with Pulmonary Sequestration: A Case Control Study.Acad Radiol. 2025 Jul;32(7):4197-4205. doi: 10.1016/j.acra.2025.05.005. Epub 2025 May 22. Acad Radiol. 2025. PMID: 40410108
-
The effect of deep learning reconstruction on abdominal CT densitometry and image quality: a systematic review and meta-analysis.Eur Radiol. 2022 May;32(5):2921-2929. doi: 10.1007/s00330-021-08438-z. Epub 2021 Dec 15. Eur Radiol. 2022. PMID: 34913104 Free PMC article.
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
References
LinkOut - more resources
Full Text Sources