

Visualized breath-hold training for reducing respiratory motion artifacts in liver dynamic contrast-enhanced magnetic resonance imaging
- PMID: 40785901
- PMCID: PMC12332653
- DOI: 10.21037/qims-2024-2526
Visualized breath-hold training for reducing respiratory motion artifacts in liver dynamic contrast-enhanced magnetic resonance imaging
Abstract
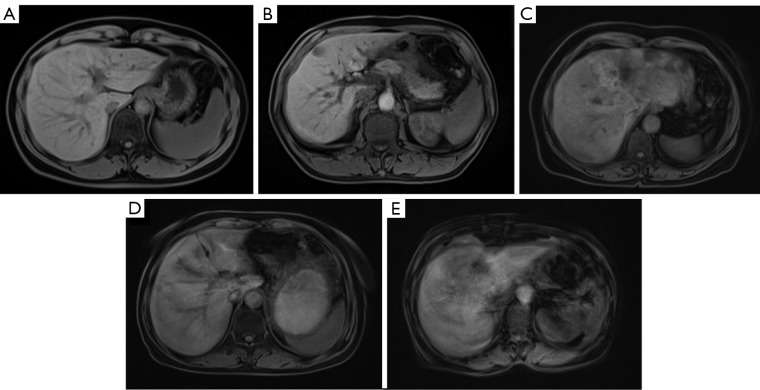
Background: Liver dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) plays a critical role in detecting hepatic lesions but is highly susceptible to respiratory motion artifacts. Although advancements in rapid magnetic resonance (MR) acquisition techniques have been made, breath-hold acquisitions are predominantly used for abdominal DCE-MRI due to their superior image quality. Therefore, prescan breath-hold training is essential to improving patients' compliance and minimizing respiratory artifacts. Traditional oral training methods, which rely on operators monitoring chest/abdominal movement, are subjective and often insufficient for DCE-MRI requirements, leading to suboptimal image quality and potential risks from repeated contrast administration. To address these limitations, we developed a novel visual breath-hold training instrument and evaluated its efficacy in reducing respiratory artifacts.
Methods: This retrospective study included 174 patients undergoing liver DCE-MRI (pre-contrast, early arterial, late arterial, portal, and parenchymal phases). Patients were divided into two groups: the visualized breath-hold training (VBT) group (n=87) and the oral breath-hold training (OBT) group (n=87). In the VBT group, breath-hold training was performed with a self-designed visualized respiration training device. Operators objectively assessed training performance and provided individual guidance. In the OBT group, conventional training, with standard verbal instructions and tactile examination of the patients' chest and abdomen, was applied. For analyzing image quality, quantitative metrics [signal-to-noise ratio (SNR) and contrast-to-noise ratio (CNR)] and qualitative respiratory artifact scores were compared between groups with the Mann-Whitney U test. For the comparison of diaphragmatic stability across sequential breath-holds, slice pages of the top or bottom of liver were recorded and analyzed via the Mann-Whitney U test. A subgroup analysis was performed on non-contrast images from 18 patients, with respiratory artifacts being scored for paired intra-individual comparisons.
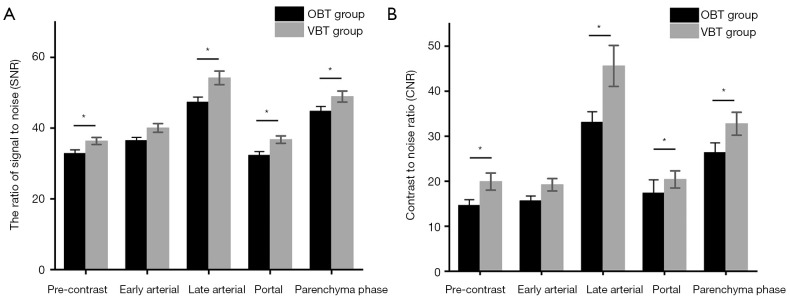
Results: The VBT group had a significantly higher SNR and CNR than did the OBT group in the pre-contrast (SNR: P=0.018; CNR: P=0.006), late arterial (SNR: P=0.016; CNR: P=0.029), portal (SNR: P=0.003; CNR: P=0.002), and parenchymal phases (SNR: P=0.044; CNR: P=0.010). Respiratory artifact scores were lower in the VBT group across all phases (pre-contrast: P=0.021; early arterial: P=0.002; late arterial: P=0.001; portal: P<0.001; parenchymal: P<0.001). Diaphragmatic consistency during sequential breath-holds was significantly higher in the VBT group between the early arterial and portal phases (P=0.046) and the late arterial and portal phases (P=0.011) as compared to the OBT group. Intra-individual subgroup analysis further confirmed the reduction of artifacts in the pre-contrast phase scans (P=0.010).
Conclusions: VBT effectively reduces respiratory motion artifacts and enhances image quality in liver DCE-MRI by improving patient compliance. This approach holds promise for optimizing clinical workflows and diagnostic accuracy, especially in populations with limited breath-hold capacity.
Keywords: Visualized breath-hold training (VBT); image quality; liver dynamic contrast-enhanced magnetic resonance imaging (liver DCE-MRI); respiratory artifacts.
Copyright © 2025 AME Publishing Company. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-2024-2526/coif). The authors have no conflicts of interest to declare.
Figures



Similar articles
-
Deep-learning reconstruction for noise reduction in respiratory-triggered single-shot phase sensitive inversion recovery myocardial delayed enhancement cardiac magnetic resonance.Magn Reson Imaging. 2025 Oct;122:110460. doi: 10.1016/j.mri.2025.110460. Epub 2025 Jul 14. Magn Reson Imaging. 2025. PMID: 40669733
-
Magnetic resonance perfusion for differentiating low-grade from high-grade gliomas at first presentation.Cochrane Database Syst Rev. 2018 Jan 22;1(1):CD011551. doi: 10.1002/14651858.CD011551.pub2. Cochrane Database Syst Rev. 2018. PMID: 29357120 Free PMC article.
-
Ultra-low-dose hepatic computed tomography with a novel real-time deep learning-based noise reduction algorithm: a prospective cross-sectional analysis of image quality and lesion detection.Quant Imaging Med Surg. 2025 Aug 1;15(8):7006-7018. doi: 10.21037/qims-2025-365. Epub 2025 Jul 24. Quant Imaging Med Surg. 2025. PMID: 40785866 Free PMC article.
-
Contrast-enhanced ultrasound using SonoVue® (sulphur hexafluoride microbubbles) compared with contrast-enhanced computed tomography and contrast-enhanced magnetic resonance imaging for the characterisation of focal liver lesions and detection of liver metastases: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2013 Apr;17(16):1-243. doi: 10.3310/hta17160. Health Technol Assess. 2013. PMID: 23611316 Free PMC article.
-
Free-Breathing High-Resolution, Swap-Free, and Motion-Corrected Water/Fat Separation in Pediatric Abdominal MRI.Invest Radiol. 2024 Dec 1;59(12):805-812. doi: 10.1097/RLI.0000000000001092. Epub 2024 Jun 10. Invest Radiol. 2024. PMID: 38857418
References
LinkOut - more resources
Full Text Sources