

Determinants and Clinical Impact of Visit-to-visit Blood Pressure Variability in Patients with Heart Failure with Preserved Ejection Fraction
- PMID: 40786446
- PMCID: PMC12328271
- DOI: 10.31662/jmaj.2024-0256
Determinants and Clinical Impact of Visit-to-visit Blood Pressure Variability in Patients with Heart Failure with Preserved Ejection Fraction
Abstract
Introduction: Blood pressure (BP) affects the prognosis of patients with heart failure with preserved ejection fraction (HFpEF). However, the implications of its variability are poorly understood. This study aimed to explore the determinants and prognostic significance of visit-to-visit BP variability (V2V-BPV) in HFpEF.
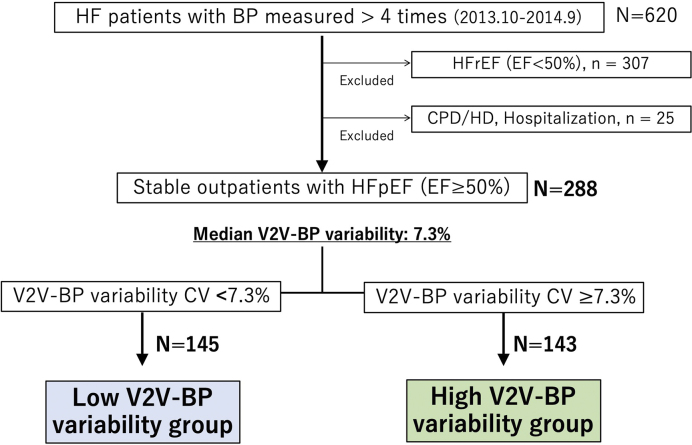
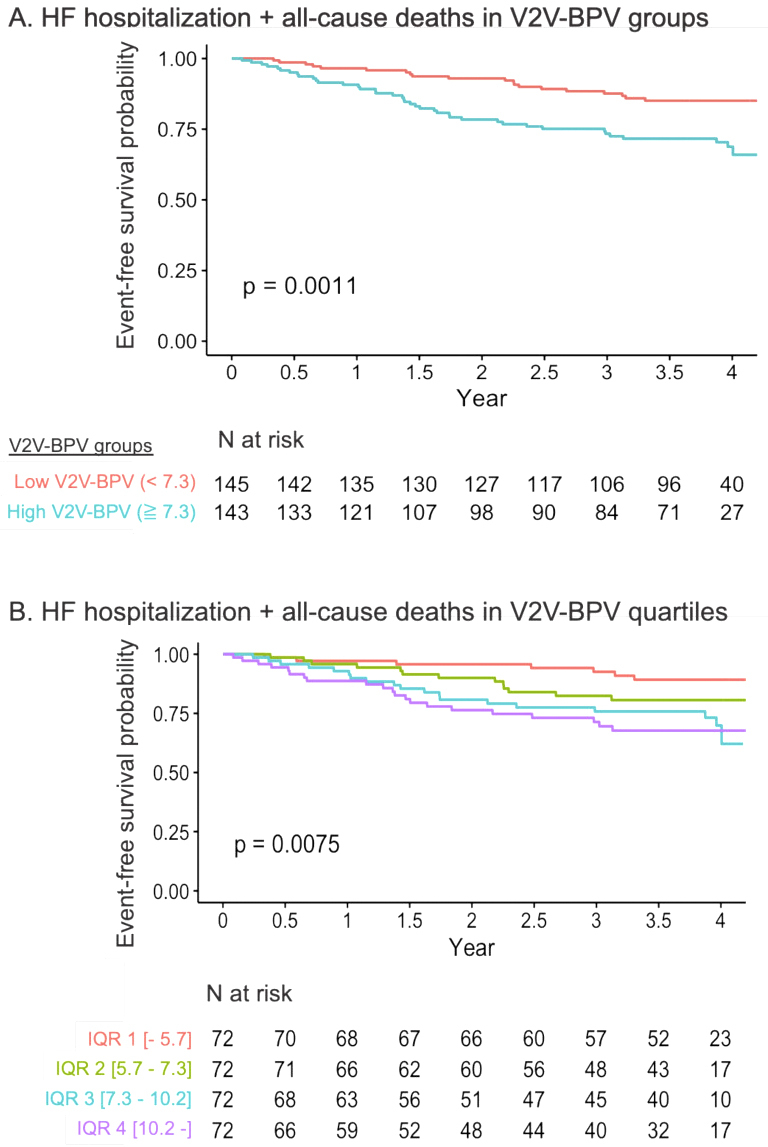
Methods: Consecutive patients with HFpEF at the Sakakibara Heart Institute of Okayama underwent routine BP measurements. V2V-BPV, calculated as the coefficient of variation of systolic BP over one year, was assessed. The primary endpoint comprised all-cause mortality and heart failure hospitalization.
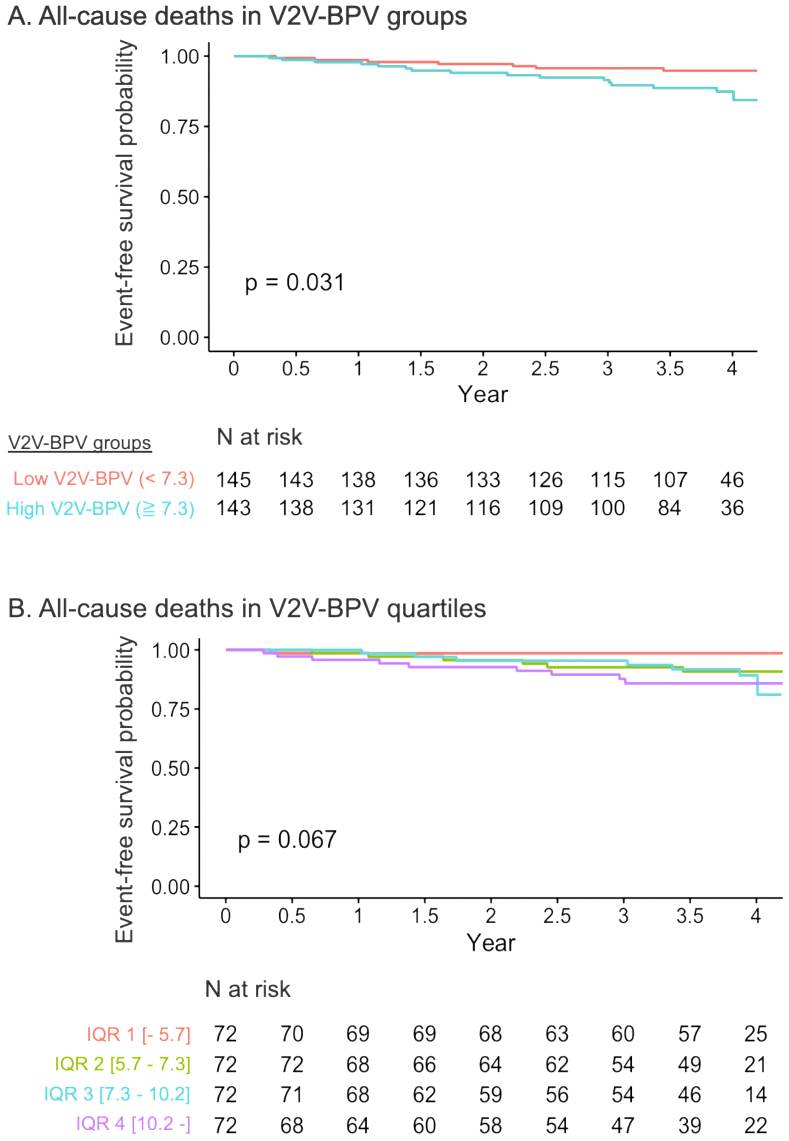
Results: Among 288 outpatients with HFpEF (average age 73 ± 10 years, 60.8% male), BP was measured 6.1 ± 1.7 times, with a median V2V-BPV of 7.3%. The high V2V-BPV group (≥7.3%) had marginally but significantly elevated B-type natriuretic peptide (BNP) levels and higher Meta-Analysis Global Group In Chronic Heart Failure risk scores (MAGGIC scores). V2V-BPV was independently associated with an increased risk of the primary endpoints (hazard ratio 1.08 per percentage point; p = 0.025), even after adjustments for systolic BP, BNP, MAGGIC score, and the number of BP measurements. A similar relationship was observed between all-cause mortality and V2V-BPV (adjusted hazard ratio 1.12, p = 0.049 with MAGGIC score). Hemoglobin level was an independent predictor of high V2V-BPV in multiple sensitivity analyses.
Conclusions: In patients with HFpEF, V2V-BPV was independently associated with adverse events, with hemoglobin level emerging as a determinant. Further research is warranted to determine whether BP stabilization can improve the prognosis of HFpEF.
Keywords: blood pressure variability; heart failure preserved ejection fraction; hypertension.
Copyright © Japan Medical Association.
Conflict of interest statement
Nobuyuki Kagiyama is affiliated with a department endowed by grants from Paramount Bed Co., Ltd., received research grants from EchoNous. Inc. and AMI Inc., and received an honorarium from Novartis Japan, Otsuka Pharma, Eli Lilly, and Nippon Boehringer Ingelheim outside the submitted work. Yuya Matsue received an honorarium from Otsuka Pharmaceutical Co., Novartis Japan, AstraZeneca K.K., Ono Pharmaceutical Co., Ltd., Kyowa Kirin Co., Ltd., Bayer Japan, and Pfizer, Inc., and research funding outside the submitted work from Nippon Boehringer Ingelheim Co., Ltd., Pfizer Inc., Otsuka Pharmaceutical Co., EN Otsuka Pharmaceutical Co., Ltd., and Roche Diagnostics Japan. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Visit-to-visit blood pressure variability and progression of white matter hyperintensities over 14 years.Blood Press. 2024 Dec;33(1):2314498. doi: 10.1080/08037051.2024.2314498. Epub 2024 Mar 13. Blood Press. 2024. PMID: 38477113
-
Post-discharge changes in nutritional status predict prognosis in patients with acute decompensated HFpEF from the PURSUIT-HFpEF Registry.Heart Vessels. 2025 Jul;40(7):577-591. doi: 10.1007/s00380-024-02499-y. Epub 2024 Dec 10. Heart Vessels. 2025. PMID: 39656282 Free PMC article.
-
Use of Spironolactone for the Treatment of Heart Failure With Preserved Ejection Fraction: Efficacy and Clinical Implications in Light of Recent Evidence.Cureus. 2025 Jun 13;17(6):e85908. doi: 10.7759/cureus.85908. eCollection 2025 Jun. Cureus. 2025. PMID: 40656394 Free PMC article. Review.
-
Association between insulin resistance indices and outcomes in patients with heart failure with preserved ejection fraction.Cardiovasc Diabetol. 2025 Jan 22;24(1):32. doi: 10.1186/s12933-025-02595-x. Cardiovasc Diabetol. 2025. PMID: 39844150 Free PMC article.
-
Sodium-glucose co-transporter 2 inhibitors in heart failure with mildly reduced or preserved ejection fraction: an updated systematic review and meta-analysis.Eur J Med Res. 2022 Dec 29;27(1):314. doi: 10.1186/s40001-022-00945-z. Eur J Med Res. 2022. PMID: 36581880 Free PMC article.
References
-
- McKee PA, Castelli WP, McNamara PM, et al. The natural history of congestive heart failure: the Framingham study. N Engl J Med. 1971;285(26):1441-6. - PubMed
-
- Dougherty AH, Naccarelli GV, Gray EL, et al. Congestive heart failure with normal systolic function. Am J Cardiol. 1984;54(7):778-82. - PubMed
-
- Vasan RS, Levy D. Defining diastolic heart failure: a call for standardized diagnostic criteria. Circulation. 2000;101(17):2118-21. - PubMed
-
- Bhatia RS, Tu JV, Lee DS, et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N Engl J Med. 2006;355(3):260-9. - PubMed
LinkOut - more resources
Full Text Sources