

Two-year longitudinal and prospective electroencephalographic follow-up in patients with TBI: can early EEG and CT findings predict post-traumatic epilepsy?
- PMID: 40786630
- PMCID: PMC12332879
- DOI: 10.3389/fneur.2025.1609733
Two-year longitudinal and prospective electroencephalographic follow-up in patients with TBI: can early EEG and CT findings predict post-traumatic epilepsy?
Abstract
Introduction: Traumatic brain injury (TBI), caused by external force to the head, leads to anatomical or functional damage to cranial structures. It is a leading cause of morbidity and mortality in adults worldwide, with substantial economic burden. Post-traumatic epilepsy (PTE) is a significant complication of TBI, posing immense challenges to rehabilitation and exacerbating socioeconomic burdens. The incidence of PTE varies widely, underscoring the need for early detection and treatment.
Objective: Through prospective electroencephalography (EEG) evaluations over a two-year period, our study aims to identify electrographic patterns indicative of PTE development, offering crucial insights for timely intervention and improved patient outcomes.
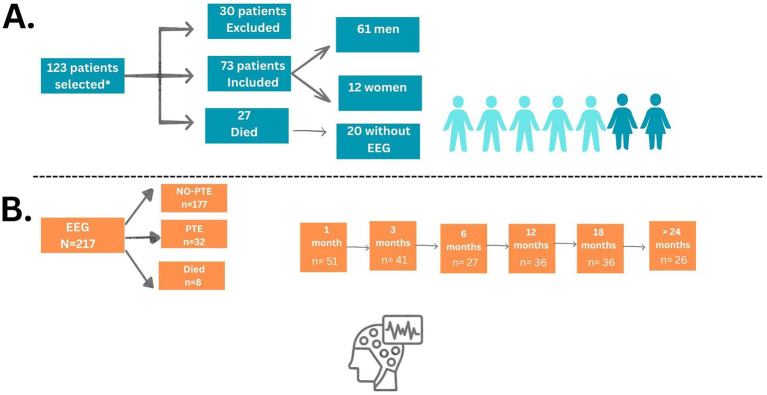
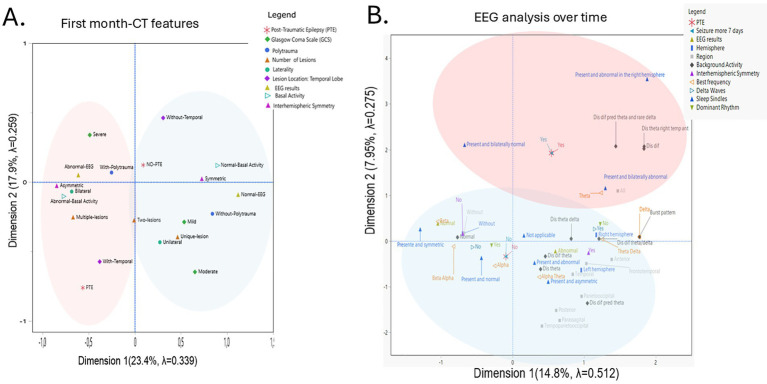
Methods: Seventy-three adult participants with acute TBI, admitted to a reference hospital in Brazil between 2018 and 2020, were recruited based on eligibility criteria. EEG evaluations monitored seizure occurrence with follow-ups for up to 24 months post-TBI, though these were disrupted by the COVID-19 pandemic. Analyses included established EEG protocols, examining factors such as background activity and epileptiform paroxysms. Relative risk (RR), Multiple Correspondence Analysis (MCA), logistic regression, and Generalized Estimating Equations (GEE) were employed to predict variables associated with PTE development.
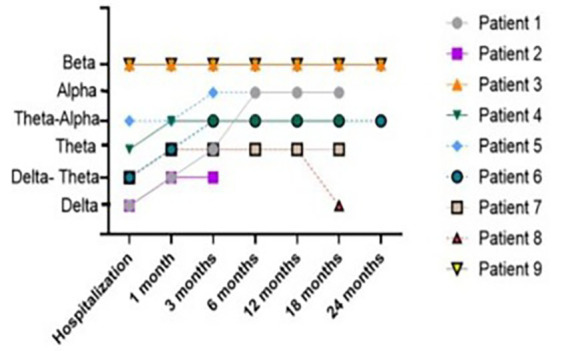
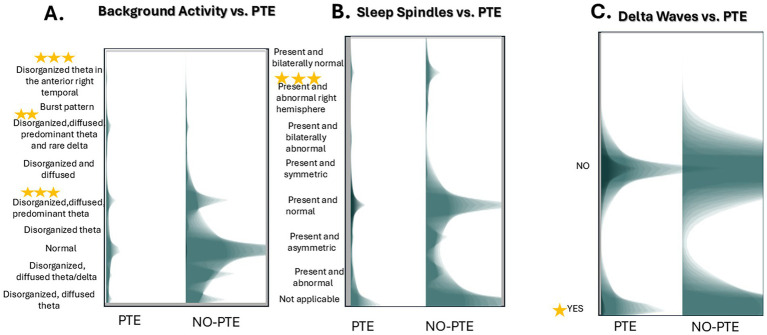
Results: Both PTE and NO-PTE (no post-traumatic epilepsy) patients showed improving background activity over 2 years. EEG recordings revealed that injuries in the temporal region, diffuse theta waves and abnormal bilateral sleep elements indicated a higher risk of PTE development. Additionally, multiple lesions were also associated with PTE.
Conclusion: This comprehensive approach provides valuable insights for clinical management and sheds light on the complex interplay of factors influencing TBI outcomes.
Keywords: EEG; biomarker; electroencephalography; post-traumatic epilepsy; seizure; traumatic brain injury.
Copyright © 2025 de Oliveira, Sanabria, Baise, Valeriano, dos Santos, Longo, Andrade, Ferreira Junior, Oshiro, Leite, Foresti, Mello and Garzon.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Predictive value of peripheral blood inflammatory markers for epilepsy occurrence in traumatic brain injury patients.Acta Epileptol. 2025 Jun 26;7(1):36. doi: 10.1186/s42494-025-00226-2. Acta Epileptol. 2025. PMID: 40571946 Free PMC article.
-
Predicting posttraumatic epilepsy using admission electroencephalography after severe traumatic brain injury.Epilepsia. 2023 Jul;64(7):1842-1852. doi: 10.1111/epi.17622. Epub 2023 May 6. Epilepsia. 2023. PMID: 37073101 Free PMC article.
-
Anti-seizure medications for neonates with seizures.Cochrane Database Syst Rev. 2023 Oct 24;10(10):CD014967. doi: 10.1002/14651858.CD014967.pub2. Cochrane Database Syst Rev. 2023. PMID: 37873971 Free PMC article.
-
Idiopathic (Genetic) Generalized Epilepsy.2024 Feb 12. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Feb 12. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 31536218 Free Books & Documents.
-
Technological aids for the rehabilitation of memory and executive functioning in children and adolescents with acquired brain injury.Cochrane Database Syst Rev. 2016 Jul 1;7(7):CD011020. doi: 10.1002/14651858.CD011020.pub2. Cochrane Database Syst Rev. 2016. PMID: 27364851 Free PMC article.
References
-
- James SL, Bannick MS, Montjoy-Venning WC, Theadom A, Ellenbogen RG, Montjoy-Venning W, et al. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:56–87. doi: 10.1016/S1474-4422(18)30415-0, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources